This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
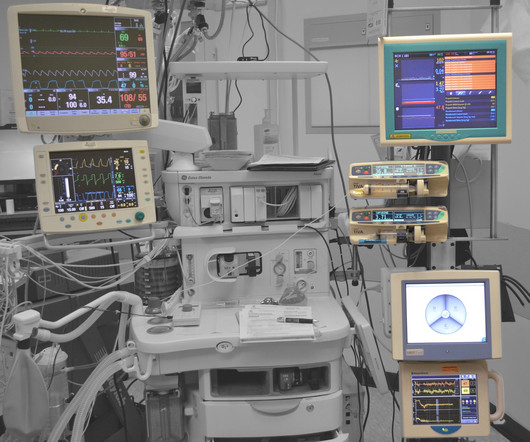
The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” A score of 40 – 60 is considered an optimal amount of anesthesia depth.
How soon will we see robotic anesthesia in our hospitals and surgery centers? But what’s new in anesthesia the last 30 years? Ten years ago, when I asked him what new anesthesia drugs were in the pipeline, he answered, “None, and there probably will be very few new ones. Is the same true for anesthesia devices?
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
The procedure does not require a breathing tube, so we’ll administer the sedation and be vigilant regarding what happens to the patient’s vitalsigns. As with all anesthetics, the patient will be fully monitored for heart rate, blood pressure, oxygen saturation, respiratory rate, and exhaled carbon dioxide level.
In an anesthetic disaster the brain can be deprived of oxygen. Without oxygen, brain cells die, and once they die they do not regenerate. Some brain cells start dying within five minutes after the oxygen supply disappears, and brain hypoxia can rapidly cause severe brain damage or death. and some don’t. and some don’t.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content