This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Just before the start of anesthesia, a patient may hear the operating room nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
Due to the differences in complexity, duration, extent of surgical trauma and postoperative pain, there are different anesthesia considerations for simple and radical hysterectomy. Preoperatively, patients requiring radical hysterectomy may present with more risk factors for anesthesia compared to those needing simple hysterectomy 3.
In choosing the most appropriate anesthesia technique, healthcare providers consider several factors to optimize patient outcomes and enhance recovery. Regional anesthesia (RA) and generalanesthesia (GA) are the two primary methods used for hip fracture surgeries.
Will you enable dying under generalanesthesia? A recent article from the United Kingdom discussed this topic of end of life anesthesia , otherwise known as “terminal anesthesia.” They request to have a general anesthetic so they are unconscious throughout the process of dying under generalanesthesia.
Demystifying Anesthesia: Answering the Top 5 Questions Anesthesia, the invisible hero of modern medicine, plays a crucial role in surgeries and medical procedures, ensuring patients are comfortable, pain-free, and safe. What is anesthesia, and how does it work? Is anesthesia safe?
Whether performed for aesthetic enhancement or medical reasons, such as correcting drooping eyelids (ptosis) or addressing eyelid mispositioning, anesthesia plays a crucial role in ensuring patient comfort and safety during surgery. Several different methods can be used to deliver local anesthesia 2.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
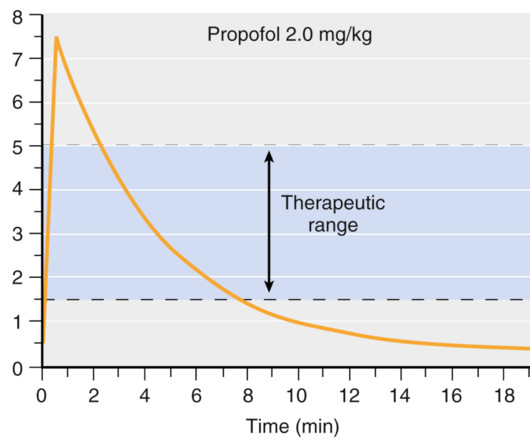
How long will the anesthesia last?” The query “How long does generalanesthesia last?” Intravenous anesthesia is well discussed in the textbook Miller’s Anesthesia , Ninth Edition , Chapter 23. Inhalational anesthesia is well discussed in the textbook Miller’s Anesthesia , Ninth Edition , Chapter 20.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? Intravenous caffeine post-surgery is not a new idea. billion dollars by 2024.
Does exposure to generalanesthesia cause dementia? Association of Mild Cognitive Impairment With Exposure to GeneralAnesthesia for Surgical and Nonsurgical Procedures: A Population-Based Study. All of their anesthesia records for surgeries after the age of 40 were reviewed. In a word, “No.” Anesthesiology.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. I’ve performed countless general anesthetics for surgeries requiring smooth emergence, specifically carotid endarterectomies, rhinoplasties, facelifts, craniotomies, thyroidectomies, and other head and neck procedures.
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation.
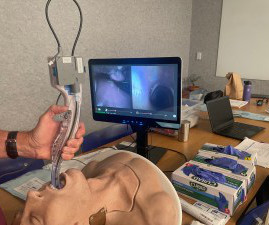
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
I’m writing this review to inform anesthesia providers and laypersons regarding developments in the field of anesthesiology. Vladimir Nekhendzy, Clinical Professor of Anesthesiology and Otolaryngology, Stanford University School of Medicine, and Past President of the Society for Head and Neck Anesthesia, is the inventor of the Spiro device.
Anesthesia plays a critical role in cesarean sections, not only to ensure the mother’s comfort and pain-free experience but also to safeguard her physiological stability and promote a positive initial bonding with the baby. However, spinal anesthesia can cause hypotension (low blood pressure), which might reduce blood flow to the fetus.
He was receiving propofol without an anesthesia professional to monitor his airway, breathing, and oxygen saturation. The package insert for propofol states: “For generalanesthesia or monitored anesthesia care (MAC) sedation, propofol should be administered only by persons trained in the administration of generalanesthesia.”
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct generalanesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
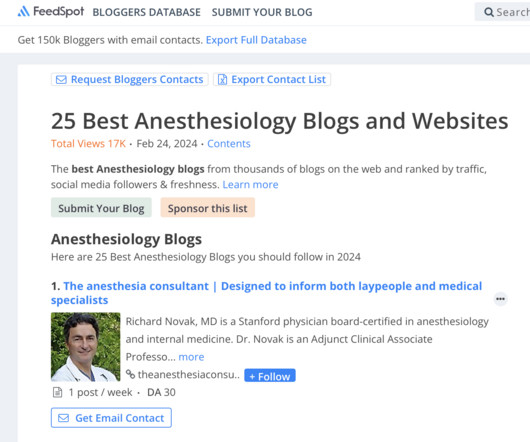
My name is Dr. Richard Novak, the author of About The Anesthesia Consultant. The Anesthesia Consultant exists to increase your knowledge about anesthesia and the practice of medicine before, during, and after surgery. This anesthesia blog contains more than 180 distinct pages and posts, all written by me.
Today theanesthesiaconsultant.com was named the #7 anesthesia blog in the world by Feedspot. See the link here to view the complete list of the world’s top anesthesia blogs. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia?
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. How does a group determine whether a potential anesthesia hire is an affable, friendly, easy-to-get-along-with individual? What Are the Common Anesthesia Medications?
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
Richard Novak, an Adjunct Clinical Professor of Anesthesiology at Stanford University Medical Center, is available for anesthesia expert witness consultation. 2020 Invited presentation via Zoom to the American Sleep Apnea Association, Sleep Apnea and Anesthesia , November 3, 2020. Yearly lecture.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? The Anesthesia Consultant’s 2022 List of the Top Anesthesia Books includes: Miller’s Anesthesia , 9th edition, 2019, Editor-in-Chief Michael Gropper.
What’s the relationship between alcohol and anesthesia? Miller’s Anesthesia , 9 th edition, Chapter 31, Preoperative Evaluation) All adults and adolescents should be questioned regarding their history of alcohol use prior to anesthesia. Why Did Take Me So Long To Wake From GeneralAnesthesia? Is this OK?
The Anesthesia Consultant was just named the #1 anesthesiology blog in the world by Feedspot. million clicks on The Anesthesia Consultant from over 100 countries. Half the articles are intended for anesthesia professionals, and half are intended for lay readers. Feedspot ranked a total of 25 anesthesia blogs/websites.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
Patients sometimes say, “Why did it take me so long to wake up after anesthesia?” Certain patients have consistent bad experiences from a past general anesthetic. They wonder if they are at increased risk for anesthesia, if something went wrong in their past anesthetics, and whether they can do about it.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? Twenty-first century general anesthetics are nearly identical to the anesthetic techniques of the late 1990s. How can it be that generalanesthesia has ceased to evolve?
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Anesthesia is a critical component of medical procedures, ensuring that patients undergo surgeries and interventions with minimal pain and discomfort. However, several myths surround the use of anesthesia, leading to misconceptions and concerns among individuals. Myth: Anesthesia always leads to unconsciousness.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
BEFORE SURGERY In every cannabis using patient, the anesthesia preoperative evaluation should include assessment of the psychologic, cardiac, and pulmonary systems in order to minimize any risk of a perioperative complication. The cannabis drugs were administered 20 minutes before induction of generalanesthesia in a double-blind fashion.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
If a patient suffers a bad outcome after anesthesia, did the anesthesiologist commit malpractice? If there was an anesthesia error, was it anesthesia malpractice? There are risks to every anesthetic and every surgery, and if a patient sustains a complication, it may or may not be secondary to substandard anesthesia care.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under generalanesthesia. Is CHATGPT as good as an MD? No, not really.
There are iPad apps to help you answer the question regarding frailty and anesthesia. My training was in both internal medicine and anesthesiology, and the intersection of these two fields is geriatric anesthesia. References: Sieber F, Pauldine R, Geriatric Anesthesia, Miller’s Anesthesia, Chapter 80, 5 th edition, 2407-2422.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. In a perfect anesthesia world, patients will not move.
This column will help you find the top 10 anesthesia journals. There are multiple fine journals in our specialty, but in my opinion the top 10 periodical anesthesia publications for clinical information follow below. Note that 2 of the top 4 publications did not even exist when I began my anesthesia training in 1984.
The capacity to deliver this much oxygen to a non-intubated patient is a marked advance in anesthesia care. We extended the apnea times of 25 patients with difficult airways who were undergoing generalanesthesia for hypopharyngeal or laryngotracheal surgery. I was—in a word—flabbergasted. Its use expanded to adult ICUs.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content