This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
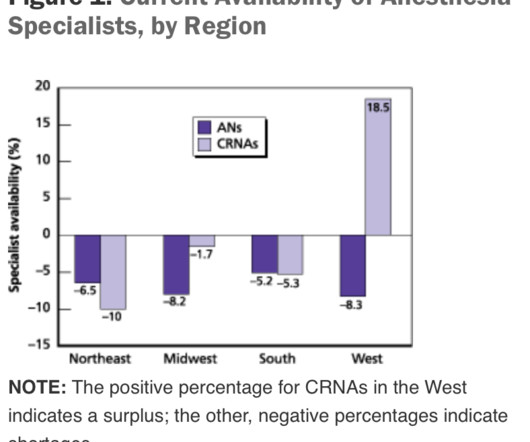
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
The incidence of cardiac arrest totally attributable to anesthesia mismanagement was low (0.47 per 10,000 anesthetics), and anesthesia mismanagement was responsible for only 1.5% 2) From 2010 to 2013 the National Anesthesia Clinical Outcomes Registry reported the risk of intraoperative cardiac arrest as 5.6 of deaths. (1)
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). (He In a word, no. No, they are not.
Anesthesia is a hands-on specialty. Anesthesia is said to be “99% boredom and 15 panic,” because 99% of the time patients are stable, yet 1% of the time, especially at the beginning and the end of anesthetics, urgent or emergency circumstances could threaten the life of the patient. Love it or hate it, the EMR is here to stay.
At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. In this model, an MD anesthesiologist supervises up to four CRNAs who work in up to four different operating rooms simultaneously. Are CRNAs and anesthesiologists equals?
What do you need to know before you start your first job following anesthesia residency? When an anesthesiologist finishes their formal training, he or she has a brain full of academic teachings, and has performed hundreds of anesthetics in a university setting while being supervised by faculty members. But are you ready to work alone?
and Maheswari et al. ) Closed-loop anesthesia computer controllers for AI titration of anesthesia level Two editorials accompany these publications. None of us wants to manage a deteriorating patient by trying to deactivate a malfunctioning computer-assisted anesthesia system, only to have it respond, ‘I’m sorry.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operating room. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia personnel will be in great demand.
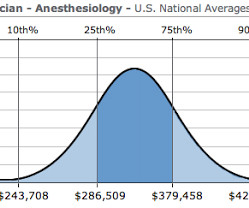
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. CRNAs can now administer anesthesia independent of any physician anesthesiologist supervision in the majority of the United States. The PGY2 year consists of all anesthesia rotations.
But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. Anesthesia providers, be they physician anesthesiologists or nurse anesthetists, are tasked with providing safe and quality anesthesia care. What is this threat? What is anesthesiology’s Achilles’ heel?
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Anesthesia Workstation You log into the EMR system, and then you log into your first patient’s chart. The lower drawers to the computerized pharmacy cart unlock, and you’re able to access the propofol you’ll use to induce anesthesia.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency. After ten minutes, he left to pursue other duties.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. In my previous essays Robot Anesthesia and Robot Anesthesia II , I described models of robots designed to perform intravenous sedation or intubation of the trachea, products which are futuristic but currently have no market share.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
Surgeons have been using trocars for generations to minimize the trauma of surgical procedures and reduce the need for anesthesia, and to help patients recover faster. The pellets produce a baseline for testosterone that can be adjusted with occasional use of patches or injections under medical supervision.
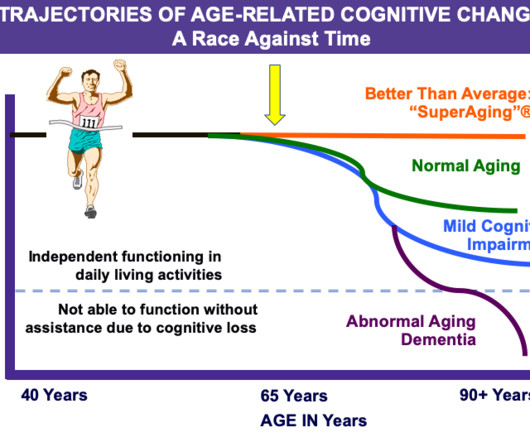
The testing includes a peer-conducted clinical skills assessment by three medical staff members, a comprehensive physical exam, and cognitive screening under supervision of the neuropsychiatry department, to address the applicant’s capacity to perform the clinical privileges requested. Why Did Take Me So Long To Wake From GeneralAnesthesia?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content