This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Just before the start of anesthesia, a patient may hear the operatingroom nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
link] Efficient Case Scheduling - Secret to a Well-Run OR Operatingroom costs can be categorized as fixed or variable. link] Efficient Case Scheduling - Secret to a Well-Run OR Operatingroom costs can be categorized as fixed or variable. While the procedure may require the use of available equipment (CT, MRI, etc.)
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. binocular Moverio BT-35E smart glasses A South Korean group led by Dr. Y.E.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. Many employers prefer hiring nurses with a BSN due to the comprehensive training they receive.
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. 1] Arora et al.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
The Realizing Improved Patient Care through Human-Centered Design in the OperatingRoom (RIPCHD.OR) learning lab uses a socio-technical approach incorporating human factors engineering and evidence-based design principles to create an optimal ergonomically sound operatingroom that results in improved patient and staff safety.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. If you purchased all 11 books in a print version today it would cost $1,643.49.
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. What do you do?
GENERAL ANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation. What do you do?
When you think of the operatingroom (OR), what comes to mind? I first learned how to scrub – setting up the instruments and handing them to the surgeon during the procedure – and then I moved into circulating, a more typical RN role of providing direct patient care before, during and after the procedure.
The operatingroom (OR) is a team based unit where patients undergo surgical procedures. Each day, they are assigned to an OR and assist with the surgeries scheduled in that room for the whole day. Typically they are a team for the whole shift or until cases are finished in that room for the day.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Anesthesia departments are crucial to the success of operatingrooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
Learjet anesthesia? Yes, anesthesia can be a glamorous specialty. Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operatingroom 13 of Stanford University Hospital.
One goal of theanesthesiaconsultant.com is to make the practice of anesthesia safer. The practice of anesthesia on healthy patients is quite safe, but we want to do everything we can to avoid preventable errors. The safety of anesthesia on ASA I and II patients has been compared to the safety record of commercial aviation.
My experience in Quality assurance/Quality improvement programs includes: Stanford University Hospital QA Committee (Care Review Committee), 1997 – 2009 Stanford University Anesthesia QA Committee, 2002 – 2009, and Waverley Surgery Center QI Committee (Chairman), 2002 – present. Mistakes happen in medicine.
The capacity to deliver this much oxygen to a non-intubated patient is a marked advance in anesthesia care. Dr. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operatingroom. At the 2023 American Society of Anesthesiologists meeting in San Francisco, I walked by a booth advertising High Flow Nasal Oxygen.
1,2 Throughout the turmoil, health systems have leaned heavily on anesthesia providers’ diverse skill set to tackle these challenges. 1,2 Throughout the turmoil, health systems have leaned heavily on anesthesia providers’ diverse skill set to tackle these challenges.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
A recent 2024 publication in JAMA looked at 8429 surgical procedures from March 2021 to December 2022 in a single institution. The anesthesiologist could indirectly visualize the patient’s vocal cords, which enabled the placement of the endotracheal tube into the windpipe. I utilize VL for difficult airway cases or emergency cases.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. Medications may need to be adjusted or temporarily stopped to minimize potential risks during the procedure. This could indicate a cardiac event or a complication related to the anesthesia.
The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” A score of 40 – 60 is considered an optimal amount of anesthesia depth.
Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. This may occur via a telephone call one day prior to surgery, or in the preanesthetic room on the day of surgery. Most of the time an anesthesiologist works in the operatingroom.
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct general anesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following general anesthesia. I tried it on several of my patients who had prolonged awakening after general anesthesia. Anesthesia was terminated 5 minutes later and the rats were placed on their backs on a table. It helps a lot!”
Anesthesia is a hands-on specialty. Picture this: your job requires you to spend the majority of your day in a windowless room with four other people. You cannot leave the room, and if you make a serious error in your work, someone can die. Since the development of the internet, anesthesia practice has changed forever.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). You take the elevator to the third floor and proceed to the locker room. The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. You leave your street clothes in your locker.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The patient consents.
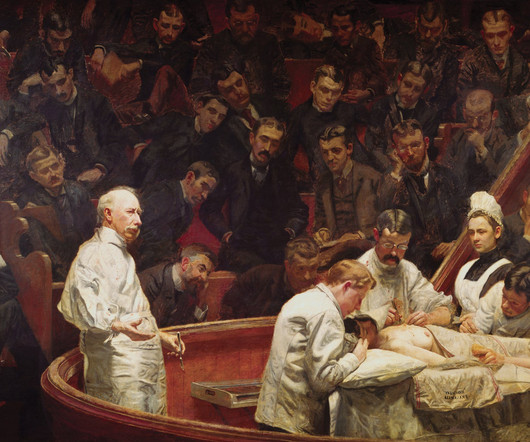
The first public demonstration of anesthesia, at the Ether Dome in Massachusetts General Hospital Important advances in the history of anesthesia changed medicine forever. Humans have inhabited the Earth for 200,000 years, yet the discovery of surgical anesthesia was a relatively recent development in the mid-1800s.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The ET tube is a conduit to safely transfer oxygen and anesthesia gases into and out of the lungs. Extubation is risky business.
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Whether it’s a heart bypass or valve replacement, these procedures require precision and teamwork. Their role is crucial for ensuring a smooth operation, but what exactly do they do, and why are they so essential in cardiovascular surgeries? Surgical assistants work closely with surgeons to ensure safe and efficient procedures.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. Why would I say this? Two anecdotes will illustrate why I understand the problem.
The Crucial Role of Surgical Assistants in Plastic Surgery Surgical assistants are indispensable in the operatingroom, handling tasks that are critical to the success of any procedure. Postoperative Care: Assisting with closing incisions, applying dressings, and ensuring patient comfort as they recover from anesthesia.
They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. Proper planning creates the best possibility for surgical procedures to go well.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. An important question for many Americans is, “Is it safe for me to have surgery during this COVID pandemic?” It depends. Everyone in the healthcare facility will be wearing masks.
You’ve found The Anesthesia Consultant website, so you have some interest in anesthesia. The truth is: a career in anesthesia involves unique demands that most people would not seek, tolerate, or ever grow accustomed to. An operatingroom emergency is not a time for screaming, temper tantrums, or freezing.
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
SCALPEL, BOUGIE, TUBE APPROACH TO CRICOTHYROIDOTOMY This week I attended an outstanding Stanford Anesthesia Grand Rounds delivered by Drs. Most anesthesia professionals have never cut into a patient’s neck, but we must own this skill if the necessity arises. In addition, barotrauma occurred in 32% of CICO emergency procedures.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency.
You’ve graduated from a residency program in which you learned the nuances of preoperative, intraoperative, and postoperative anesthesia practice. You believe the patient is high risk in terms of his airway, his breathing, his cardiac status, and his potential for post-operative complications. You’re a board-certified anesthesiologist.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content