This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
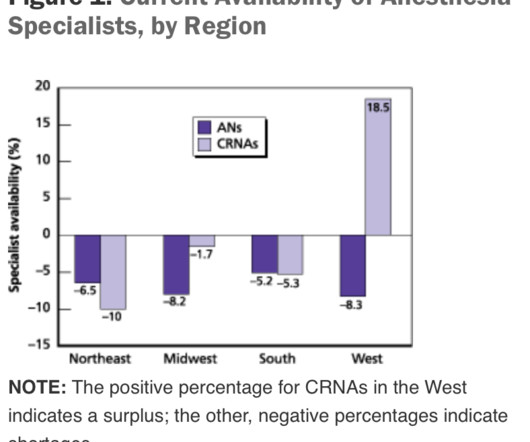
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
All APRNs are registered nurses who have earned a graduate degree that certifies them to practice advanced and specialized care. There are four classes of APRNs: certified nurse midwife (CNM), clinical nurse specialist (CNS), certified nurse practitioner (CNP), and certified registered nurse anesthetist (CRNA).
Will it be a nurse or will it be a physician? At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. All the responsibility in the ACT model resides with the supervising MD anesthesiologist. No, they are not.
to improve the bottom line, changes to the existing anesthesia staffing model may help. link] The Three Anesthesia Staffing Models: The optimal hospital staffing model should: 1. support clinical excellence Let’s look at the three most common staffing models for anesthesia delivery in the United States: 1. add revenue streams 3.
What’s the difference between a physician anesthesiologist and a nurse anesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurse anesthetist? The answer: internal medicine.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
The incidence of cardiac arrest totally attributable to anesthesia mismanagement was low (0.47 per 10,000 anesthetics), and anesthesia mismanagement was responsible for only 1.5% 2) From 2010 to 2013 the National Anesthesia Clinical Outcomes Registry reported the risk of intraoperative cardiac arrest as 5.6 of deaths. (1)
What do you need to know before you start your first job following anesthesia residency? When an anesthesiologist finishes their formal training, he or she has a brain full of academic teachings, and has performed hundreds of anesthetics in a university setting while being supervised by faculty members. But are you ready to work alone?
As a registered nurse, you would think that all this technology supporting the hiring process of nurses would lead to improvements or faster response times but if you have ever spent time on a single application website then you know the frustration and effort that simply goes to waste. What a disaster?!
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Since the development of the internet, anesthesia practice has changed forever. Love it or hate it, the EMR is here to stay.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. No, it’s not the nurse anesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. What is this threat?
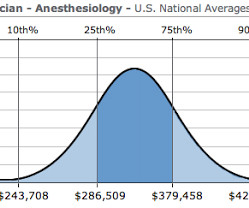
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia has never been safer.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Anesthesia Workstation You log into the EMR system, and then you log into your first patient’s chart. The lower drawers to the computerized pharmacy cart unlock, and you’re able to access the propofol you’ll use to induce anesthesia.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. In my previous essays Robot Anesthesia and Robot Anesthesia II , I described models of robots designed to perform intravenous sedation or intubation of the trachea, products which are futuristic but currently have no market share.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency. After ten minutes, he left to pursue other duties.
During this time, they receive hands-on experience in various surgical procedures under the supervision of experienced surgeons. Postoperative care also includes working with other healthcare professionals, like nurses and physical therapists, to promote a smooth recovery 5,6. What are the surgical specialties? ACS [link] 9.
20, 2025 /PRNewswire/ -- Certified registered nurse anesthetists (CRNAs) are usually the last person a patient sees before a surgical procedure begins, and the first person they awake to when it ends. As the hands-on providers of anesthesia, CRNAs are with their patients throughout the entire medical procedure. HARRISBURG, Pa.,
I’d already secured my medical staff privileges and my appointment to the anesthesia service. At Stanford every nurse, doctor, and janitor knew my name. Heidi, this is Dr. Nicolai Antone, a welcome addition to the anesthesia staff. Nico, I want you to meet Bobby Dylan, our Director of NurseAnesthesia,” Perpich said.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content