This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It’s a path that demands not only clinical excellence but also a significant shift in roles—from direct patient care in a high-intensity setting to the precision and autonomy of anesthesia. Understanding the Shift The transition from ICU to operating room (OR) involves a fundamental change in responsibilities.
Just before the start of anesthesia, a patient may hear the operating room nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Since this historic milestone, advancements in anesthesia administration and newer anesthetics led to the medical specialty of anesthesiology in the early 20th century. 1824 – Henry Hill Hickman (1800-1830) describes carbon dioxide anesthesia for animals. 4000 BCE – Sumerian artifacts depict opium poppy ca.
For patients with restless leg syndrome undergoing anesthesia, the involuntary leg movements and discomfort can pose challenges for anesthesiologists, requiring specialized techniques and considerations to ensure safe and effective anesthesia administration.
I’m writing this review to inform anesthesia providers and laypersons regarding developments in the field of anesthesiology. Vladimir Nekhendzy, Clinical Professor of Anesthesiology and Otolaryngology, Stanford University School of Medicine, and Past President of the Society for Head and Neck Anesthesia, is the inventor of the Spiro device.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
Anesthesiology residents play an important role in the operating room (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
Happy CRNA Week 2024 A lot has happened The last two months I moved to San Diego Oh what joyous fun A lot of changes for my family and for me New preschool, grandparent help, New workplace A lot of things to learn “Reprogramming” I’d like to say Each NORA (Non-Operating Room Anesthesia) location Different than the next A lot of new people More than (..)
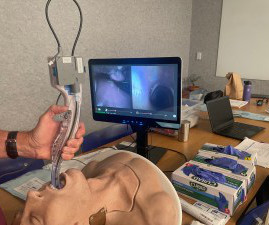
In the smart glasses group, the ultrasound machine was located behind the operator, and the smart glasses were paired with the ultrasound machine. Would the addition of smart glasses for routine monitoring be an overdose of technology in the operating room cockpit? Does excessive technology distract us from the actual patient?
Anesthesia plays a critical role in cesarean sections, not only to ensure the mother’s comfort and pain-free experience but also to safeguard her physiological stability and promote a positive initial bonding with the baby. However, spinal anesthesia can cause hypotension (low blood pressure), which might reduce blood flow to the fetus.
Pre-operative anxiety , the psychological distress which patients experience that is provoked by concerns related to their surgical and anesthetic care, 1 is estimated to affect up to 75% of children 2 and 80% of adult patients. 3,4 It has been linked to multiple intra-operative and post-operative complications (e.g.,
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operating room? Why Did Take Me So Long To Wake From General Anesthesia?
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
GENERAL ANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation. What do you do?
Recognizing frailty in anesthesia patients is critical. What if your patients, especially elderly patients, could enter their personal data and symptoms into an iPad app, and what if that information could help you determine if their risk for anesthesia was too great to risk having surgery? Can you imagine this?
My experience in Quality assurance/Quality improvement programs includes: Stanford University Hospital QA Committee (Care Review Committee), 1997 – 2009 Stanford University Anesthesia QA Committee, 2002 – 2009, and Waverley Surgery Center QI Committee (Chairman), 2002 – present. The patient had an immediate cardiac arrest.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
[link] Efficient Case Scheduling - Secret to a Well-Run OR Operating room costs can be categorized as fixed or variable. Variable costs are largely driven by caseload and associated labor costs that occur outside of normal operational hours. Fixed costs include such things as a mortgage, administration, and salaried employee costs.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operating room.
Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operating room suite. All anesthesia providers should have access to the current two-volume 3112-page edition.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Trauma is the most common indication for surgery and anesthesia of an acutely intoxicated individual, but other types of surgical emergencies can result from drug misuse, including vascular dissection and hemorrhagic complications linked to certain stimulants. The CAGE questionnaire can be used to this end. References 1.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Anesthesia departments are crucial to the success of operating rooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under general anesthesia. This could indicate a cardiac event or a complication related to the anesthesia.
Without a doubt, the operating room (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. Still, with the OR a prime revenue-generator for any hospital, its operation should be scrutinized to see where cost-savings might be implemented. So, why aren’t hospitals developing and expanding the OR?
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? How can it be that general anesthesia has ceased to evolve? What about regional anesthesia? Anesthesia in 2018 is markedly different from anesthesia in the 1990s.
Patients sometimes say, “Why did it take me so long to wake up after anesthesia?” They wonder if they are at increased risk for anesthesia, if something went wrong in their past anesthetics, and whether they can do about it. Anesthesia and Analgesia. ” when they discussed their previous anesthetic history.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following general anesthesia. I tried it on several of my patients who had prolonged awakening after general anesthesia. Anesthesia was terminated 5 minutes later and the rats were placed on their backs on a table.
Learjet anesthesia? Yes, anesthesia can be a glamorous specialty. Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operating room 13 of Stanford University Hospital.
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From General Anesthesia?
This month’s issue of Anesthesiology , our specialty’s leading journal, contains two studies on further incremental Artificial Intelligence in Medicine advances in the operating room. and Maheswari et al. ) Closed-loop anesthesia computer controllers for AI titration of anesthesia level Two editorials accompany these publications.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
One goal of theanesthesiaconsultant.com is to make the practice of anesthesia safer. The practice of anesthesia on healthy patients is quite safe, but we want to do everything we can to avoid preventable errors. The safety of anesthesia on ASA I and II patients has been compared to the safety record of commercial aviation.
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct general anesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
There are iPad apps to help you answer the question regarding frailty and anesthesia. My training was in both internal medicine and anesthesiology, and the intersection of these two fields is geriatric anesthesia. References: Sieber F, Pauldine R, Geriatric Anesthesia, Miller’s Anesthesia, Chapter 80, 5 th edition, 2407-2422.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. In each of these surgeries, the surgeon has an intense interest in a gentle anesthesia wake-up, free of coughing, bucking, or hypertension. His question prompted me to write this column. to 25 μg/kg/hr.”
This column will help you find the top 10 anesthesia journals. There are multiple fine journals in our specialty, but in my opinion the top 10 periodical anesthesia publications for clinical information follow below. Note that 2 of the top 4 publications did not even exist when I began my anesthesia training in 1984.
The capacity to deliver this much oxygen to a non-intubated patient is a marked advance in anesthesia care. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operating room. Widespread adoption of HFNO as routine therapy in the operating room is still lacking. I was—in a word—flabbergasted.
Like midazolam (a common anesthetic adjunct), remimazolam is a benzodiazepine and operates by modulating γ-aminobutyric acid (GABA) receptor activity to induce cell membrane hyperpolarization, thereby inhibiting neural activity via an increase in chloride ion influx (2). In the initial phase I study, remimazolam (0.01-0.30 hrs and 3.62
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content