This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The University of Michigan paper stated, “this study primarily analyzed physician-CRNA teams, the dominant practice model in US anesthesiology.”
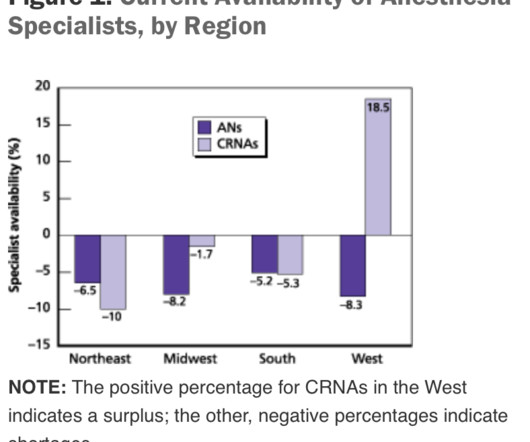
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurse anesthetists, and 3,200 anesthesiologist assistants.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). Are CRNAs and anesthesiologists equals?
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The anesthesiologist meets the patient prior to the surgery, reviews the chart, and examines the patient.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Every hospital operatingroom is equipped with a computer connected to the internet.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade.
Today I read a thoughtful and well-written essay in Anesthesiology News titled, Anesthesiologists-The Utility Players of the Medical Field written by anesthesiologist David Stinson MD from my native state of Minnesota. To me, the appropriate headline should read, “Anesthesiologists—the Most Valuable Players of the Medical Team.”
During the dayshift, working alone is seldom an issue for any anesthesiologist. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. Unlike Alex Honnold, the anesthesiologist is not putting their own life at risk—rather it is their patient who is at risk. Working alone may be less safe.
Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. A board-certified physician anesthesiologist is therefore validated as an expert in all areas of perioperative medicine. Most anesthetics are conducted by physician anesthesiologists. Are CRNAs and anesthesiologists equals?
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. CRNA Only Under this model, anesthesia care is delivered by CRNAs independently, without the involvement of an anesthesiologist. This model offers an intermediate level of costs.
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operatingroom. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
Items 1 – 5 are discussed as follows: Non-anesthesiologists can reverse the effects of remimazolam with flumazenil if they overdose a patient, but this advantage is less important for anesthesia professionals. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent.
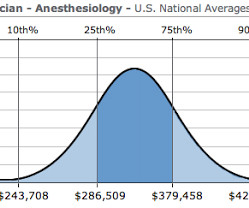
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation. The anesthesiologist decided to extubate the trachea at that time. Extubation is risky business. The patient began to cough.
Dawn Bent, DNP, MSN, CRNA , didn’t choose to be a nurse anesthetist as much as the profession chose her. She was working as an ICU nurse for eight years when one of the anesthesiologists that she worked with told her: “I think you would be a great nurse anesthetist.”
Lauren] debriefed me on how the days would go, the logistics of the surgeries — two operatingrooms were run simultaneously, and I had to monitor both rooms at once. “[They] personally asked me if I’d be interested in attending,” said Devon. “As As this was a unique opportunity that does not come along often, I said yes!
Is it feasible that CHATGPT, this decades artificial intelligence wunderkind, can equal or better a physician anesthesiologist? The surgical team will be assembled, and the child will be transferred to the operatingroom for further assessment and management. Is CHATGPT as good as an MD? No, not really.
The entire OR 1 crew – Tori, CRNA; Kristen, RNFA; Me; Shannon, CST Linda, Kristen, Shannon, Marcia (anesthesiologist), and me Tori was a great CRNA to work with! No other case was as rough as that one, and by the end of the week, we were a well-oiled machine. It was an impressive transformation to observe.
These three words make any anesthesiologist cringe. The topic of anoxic encephalopathy as related to anesthesia disasters and brain death—a issue that can ruin both a patient’s life and an anesthesiologist’s career—is not specifically covered in Miller’s Anesthesia. The anesthesiologist decided to extubate the trachea.
by PennLive.com Patients undergoing surgery or procedures requiring anesthesia are safe when cared for by a physician anesthesiologist, a certified registered nurse anesthetist (CRNA), or both. 3) relates to outdated and restrictive laws that prevent CRNAs from practicing to their fullest scope. Published: Jan.
I entered the hallway of the operatingroom complex. Hibbing General had only six operatingrooms, compared to the 40 rooms at Stanford. My old med school classmate, Michael Perpich, the Chief of Staff at Hibbing General, was the surgeon working in operatingroom #1. Nice to meet you,” I said.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content