This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
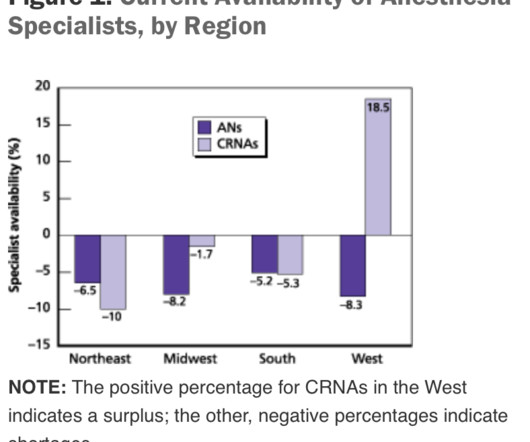
The regulation of the number of MD residency and CRNA training positions, and the duration of time required to train new professionals, impede the ability to rapidly increase the supply of clinicians entering the workforce. The net decrease in MD anesthesiologists was 2500 – 1900 = 600.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). Are CRNAs and anesthesiologists equals?
What’s the difference between a physician anesthesiologist and a nurse anesthetist? There is no fork in the career path that makes a busy Certified Registered Nurse Anesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. It’s not my intention to demean or minimize the role of CRNAs.
All MD In this model, (most prevalent in one-or two-room surgery centers and less common in large ambulatory surgery centers), all anesthesia care is provided by medical doctors only, specifically physician anesthesiologists. The benefits of this model are that there are fewer providers involved and less supervision needed.
A board-certified physician anesthesiologist is therefore validated as an expert in all areas of perioperative medicine. Most anesthetics are conducted by physician anesthesiologists. In this model, an MD anesthesiologistsupervises up to four CRNAs who work in up to four different operating rooms simultaneously.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., To the contrary, in our practice we physician anesthesiologists start the IVs ourselves.
During the dayshift, working alone is seldom an issue for any anesthesiologist. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. Unlike Alex Honnold, the anesthesiologist is not putting their own life at risk—rather it is their patient who is at risk. Working alone may be less safe.
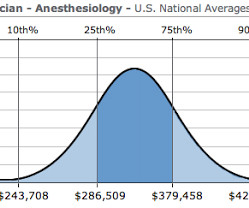
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved. Anesthesiologists in our practice telephone their patients the night before to discuss the anesthesia care. Are the majority of anesthetists MDs or CRNAs, or is the staff a mix of both? It doesn’t have to be this way.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. These devices enable an anesthesiologist to remain connected to the outside world during surgery.
At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation. The anesthesiologist decided to extubate the trachea at that time. Extubation is risky business. The patient began to cough.
These three words make any anesthesiologist cringe. The topic of anoxic encephalopathy as related to anesthesia disasters and brain death—a issue that can ruin both a patient’s life and an anesthesiologist’s career—is not specifically covered in Miller’s Anesthesia. The anesthesiologist decided to extubate the trachea.
20, 2025 /PRNewswire/ -- Certified registered nurse anesthetists (CRNAs) are usually the last person a patient sees before a surgical procedure begins, and the first person they awake to when it ends. As the hands-on providers of anesthesia, CRNAs are with their patients throughout the entire medical procedure. HARRISBURG, Pa.,
He was an anesthesiologist in California, but now he’s one of us, the slightly-better-than-average staff of Hibbing General. Why the ingratiating attitude toward me, a board-certified anesthesiologist physician? We have a full staff, like any other community hospital, but we’re light on anesthesiologists. I was miffed.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content