This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The anesthesiologist meets the patient prior to the surgery, reviews the chart, and examines the patient.
Salem Anesthesia is fortunate to have the best Anesthesiologists on our team. Their education, training and expertise is impressive and very appreciated by our surgical centers, CRNA s and patients. A vital member of this team is the anesthesiologist. A vital member of this team is the anesthesiologist.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). Are CRNAs and anesthesiologists equals?
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The University of Michigan paper stated, “this study primarily analyzed physician-CRNA teams, the dominant practice model in US anesthesiology.”
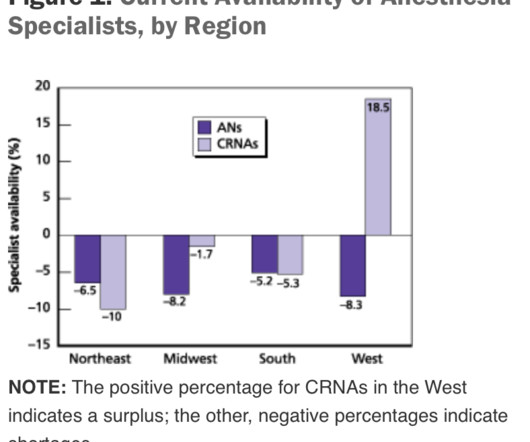
Non-emergency surgery may be delayed for days, weeks, or longer. The regulation of the number of MD residency and CRNA training positions, and the duration of time required to train new professionals, impede the ability to rapidly increase the supply of clinicians entering the workforce.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
What’s the difference between a physician anesthesiologist and a nurse anesthetist? There is no fork in the career path that makes a busy Certified Registered Nurse Anesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. It’s not my intention to demean or minimize the role of CRNAs.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring.,
You’re an anesthesiologist. I’d like to focus on one specific aspect of this important study: anesthesiologists need to lose their reluctance to cut a surgical airway into a patient’s neck in a “can’t intubate, can’t oxygenate” airway emergency. Case 5: “The anesthesiologist asked the surgeon to perform an emergency cricothyrotomy.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade. This week U.S.
Who is responsible for your safety before, during, and after your surgery? The word “perioperative” means “around the time of surgery.” It’s officially defined as the 30-day time period following surgery. Note this data was for inpatient surgeries. Who will take care of you before, during, and after YOUR surgery?
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operating room. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
During the dayshift, working alone is seldom an issue for any anesthesiologist. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. Unlike Alex Honnold, the anesthesiologist is not putting their own life at risk—rather it is their patient who is at risk. The degree of risk is variable.
Today I read a thoughtful and well-written essay in Anesthesiology News titled, Anesthesiologists-The Utility Players of the Medical Field written by anesthesiologist David Stinson MD from my native state of Minnesota. To me, the appropriate headline should read, “Anesthesiologists—the Most Valuable Players of the Medical Team.”
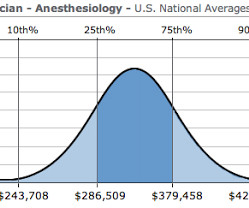
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
While few administrators would consider reducing the number of surgeries (that would strangle the golden goose!) All MD In this model, (most prevalent in one-or two-room surgery centers and less common in large ambulatory surgery centers), all anesthesia care is provided by medical doctors only, specifically physician anesthesiologists.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. These devices enable an anesthesiologist to remain connected to the outside world during surgery.
At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). After a surgery is finished, anesthetic gases and intravenous anesthesia drugs are discontinued, and the patient wakes up within 5 to 15 minutes. Extubation is not a time to relax.
The cooperation between surgeons, anesthesiologists, and internal medicine specialists to develop the protocols has been outstanding, the standardized checklist care has been well accepted, and patients are benefiting. This group would cover a hospital or several hospitals along with nearby surgery centers and offices. Grade = C-.
Items 1 – 5 are discussed as follows: Non-anesthesiologists can reverse the effects of remimazolam with flumazenil if they overdose a patient, but this advantage is less important for anesthesia professionals. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent.
These three words make any anesthesiologist cringe. If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. A 40-year-old male presented for outpatient septoplasty surgery.
Lauren] debriefed me on how the days would go, the logistics of the surgeries — two operating rooms were run simultaneously, and I had to monitor both rooms at once. The team consisted of two surgeons, an anesthesiologist, a CRNA, an internal medicine physician, four registered nurses, an instrumentation/implant rep, and myself (IONM).”
Is it feasible that CHATGPT, this decades artificial intelligence wunderkind, can equal or better a physician anesthesiologist? What sort of preoperative tests or therapies should this patient have before surgery? They will consider her individual medical history and unique circumstances to ensure a safe and successful surgery.
I was so impressed with the team from One World Surgery (OWS). Let the surgeries begin! The entire OR 1 crew – Tori, CRNA; Kristen, RNFA; Me; Shannon, CST Linda, Kristen, Shannon, Marcia (anesthesiologist), and me Tori was a great CRNA to work with! This was a great group of people!
by PennLive.com Patients undergoing surgery or procedures requiring anesthesia are safe when cared for by a physician anesthesiologist, a certified registered nurse anesthetist (CRNA), or both. 3) relates to outdated and restrictive laws that prevent CRNAs from practicing to their fullest scope. Published: Jan.
The faded turquoise tile on the walls had witnessed thousands of hernia surgeries. He was an anesthesiologist in California, but now he’s one of us, the slightly-better-than-average staff of Hibbing General. Why the ingratiating attitude toward me, a board-certified anesthesiologist physician? anesthesiologist in town.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content