This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
“You will be asleep for your surgery,” anesthesiologists often reassure their patients. Just before the start of anesthesia, a patient may hear the operatingroom nurse saying, “Think of a nice dream as you go off to sleep.” Under generalanesthesia, patients do not dream.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will future anesthesiologists routinely use caffeine to wake patients after surgery? Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic?
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. The dentist and an anesthesiologist were both present. What do you do?
Anesthesiologists aren’t well known to most patients, but these specialty doctors have certain traits in common. Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. Most of the time an anesthesiologist works in the operatingroom.
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
What are the personal characteristics of a successful anesthesiologist? You’ve found The Anesthesia Consultant website, so you have some interest in anesthesia. Perhaps you’ve heard that anesthesiologists earn a comfortable living. Anesthesiologists’ salaries are among the highest of all U.S. professions.”
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). Are CRNAs and anesthesiologists equals?
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesiaanesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation.
What’s the most critical technical skill for an anesthesiologist? I ask this question when I’m teaching anesthesia residents and medical students. The most critical technical skill for an anesthesiologist is. The American Society of Anesthesiologists Difficult Airway Algorithm addresses this issue.
What qualities define an outstanding anesthesiologist? A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. This can be a vain conceit. Be prepared.
The most significant anesthesiologist of the 20 th century died just weeks ago, on December 21, 2017. Many of you have never heard of Dr. New, and don’t know what he was famous for, but in my opinion he was the Most Valuable Player of the anesthesia ranks in the last one hundred years. His name was William New, MD, PhD.
This technology, once it’s perfected and approved for use in humans, will do what I once thought was all but impossible—it enables a device to intubate the trachea without any anesthesiologist input. No anesthesiologist wants to resort to cricothyrotomy to save a patient’s life. Sound unbelievable?
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Anesthesia emergencies are anxiety-producing for both experienced and inexperienced anesthesiologists, but experienced doctors are more likely to know exactly what to do and what not to do. Perioperative” means “the time around an operation”—specifically the preoperative, postoperative, and intraoperative times.
You’re a board-certified anesthesiologist. You’ve graduated from a residency program in which you learned the nuances of preoperative, intraoperative, and postoperative anesthesia practice. Individuals would never board a Boeing 787 aircraft and tell the pilot what to do, but individuals will try to influence their anesthesiologist.
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
Most patients have no real idea what anesthesiologists do. Most college premed students have no real idea what anesthesiologists do. Most medical students have no real idea what anesthesiologists do. Anesthesiologists are responsible for your medical care before, during, and after surgeries.
Do you know the intersection between an anesthesiologist and the NFL? Was there an anesthesiologist involved in Damar Hamlin’s resuscitation? This Airway Management Physician is most commonly an anesthesiologist or an emergency medicine physician. No anesthesiologist or emergency room physician was present.
” Despite this, during surgery your anesthesiologist injected fentanyl into your IV as part of your anesthetic. As a street drug, fentanyl overdose is a critical problem in the United States, but anesthesiologists administer fentanyl to most patients, and do so safely. Why do anesthesiologists utilize fentanyl?
A French anesthesiologist was accused of poisoning patients to trigger cardiac arrests during surgery. He worked as an anesthesiologist in the eastern French city of Besançon. The IV line is the route in which anesthesiologists inject drugs into the patient’s bloodstream to induce sleep. Nine patients died.
Anesthesiologists work in hospitals, and when a hospital closes, anesthesiologists lose their jobs. What about anesthesiologists in the current healthcare systems? There are 46,000 anesthesiologists in the U.S, and these anesthesiologists provide $20 billion worth of health care services each year.
Will Gawande change the future for anesthesiologists? Let’s look at these three proposed Gawande changes, and how they affect the future for anesthesiologists: Taking out the trash. This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals.
At one New York medical center, intense clinical demands and provider fatigue have inspired one anesthesiologist to push the boundaries of clinical medicine. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% How can an anesthesiologist make such an error? He’s right. What happened?
Today I read a thoughtful and well-written essay in Anesthesiology News titled, Anesthesiologists-The Utility Players of the Medical Field written by anesthesiologist David Stinson MD from my native state of Minnesota. To me, the appropriate headline should read, “Anesthesiologists—the Most Valuable Players of the Medical Team.”
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. The patient must wake up (when the surgery is over).
During the dayshift, working alone is seldom an issue for any anesthesiologist. A typical hospital will have dozens of other anesthesia providers working in the same building. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. There are multiple different models of anesthesia care.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
The challenges and stressors anesthesia professionals face every day are seemingly unknown to the media and the populace. Every surgical patient requires the utmost in vigilance from their physician anesthesiologist in order to prevent life-threatening disturbances of Airway-Breathing-Circulation. Read through this list.
An anesthesia emergency occurs without warning. As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You need the ultimate anesthesia emergency guidebook. Anesthesia practice is described as 99% boredom and 1% panic.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. You will wear a mask in the preoperative room, and that mask will remain on your face until just prior to the induction of anesthesia.
The two hospital guards and the mother donned white operatingroom coveralls. At the mother’s consent, the guards laid the patient down on the hospital gurney, held him there, and the surgical team and the guards pushed the gurney down the hallway to the operatingroom (a significant distance of approximately 100 yards).
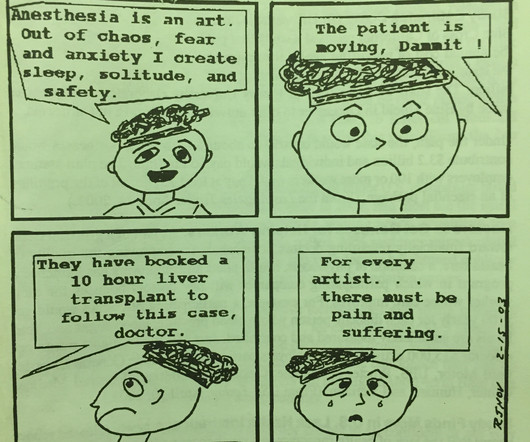
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them.
Why should anesthesiologists be any different? A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. Employees of whom?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content