This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Table of Contents What Is Hospital Surgical Support? From sterile processing and perfusion services to intraoperative neuromonitoring (IONM) and surgical assistants, hospital surgical support teams are the unsung heroes behind every successful operation. What Is Hospital Surgical Support? Surgical First Assistants 5.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
In almost every hospital the OR is the “lion”, bringing in the largest share of revenue (as much as 70%) - and eating up a large share (an estimated 40%) of a hospital’s total expenses. link] Efficient Case Scheduling - Secret to a Well-Run OR Operatingroom costs can be categorized as fixed or variable. link] Permalink
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. Evolution of Procedures and Procedural Areas Procedures that used to be hospital-based have increasingly moved into outpatient settings and physician’s offices. Imagine this: It’s the year 2034.
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You take the elevator to the third floor and proceed to the locker room.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. A doctor or a nurse?
What qualities define an outstanding anesthesiologist? Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Rather, I’m choosing to list the qualities I’ve witnessed that make physician anesthesiologists stand out as leaders.
We also had the President of the New York State Society of Anesthesiologists, Dr. Jason Lok, and Dr. John Fiadjoe, Executive Vice Chair of Anesthesia at Boston Children’s Hospital and Director of the American Board of Anesthesiology, joining us at the conference. Attendees for the annual meeting even stayed until the end on Sunday!
Imagine you’re two months out of anesthesia training, working at a community hospital, and at 2 a.m. Anesthesia emergencies are anxiety-producing for both experienced and inexperienced anesthesiologists, but experienced doctors are more likely to know exactly what to do and what not to do. This observation is no surprise.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade.
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
New York, NY – The era of COVID-19 has pushed the envelope in hospitals across the world, challenging care delivery models and allowing one ventilator to ventilate 600 patients at once. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
You utilize the current multimodal strategies for operatingroom anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% He wants to get out of bed, walk as much as possible, and go home from the hospital as soon as he can. How can an anesthesiologist make such an error?
Dr. Gawande is a Professor of Surgery at Harvard/ Brigham and Women’s Hospital, and is the bestselling author of multiple nonfiction books directed at healthcare topics. Will Gawande change the future for anesthesiologists? If an anesthesiologist wanted to use the nerve block, the insurer would not reimburse those costs.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. So, why aren’t hospitals developing and expanding the OR? link] The Three Anesthesia Staffing Models: The optimal hospital staffing model should: 1. improve efficiencies 2.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The required parts are an operatingroom anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps. The video is posted here.
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. Anesthesiologists win the tally for most operatingroom hours per week.
Imagine this: I’m a brand new attending critical care anesthesiologist in a major academic medical center and in an effort to make up for the opportunity costs of becoming a doctor, I willingly take on a very aggressive clinical schedule. Cases that most hospitals would not dare to touch. I guess I actually know a few things!
Peter, MN – Physician on FIRE , an anesthesiologist and financial blogger , recently hit the magical goal of Financial Independence and Retire Early (FIRE) in his mid 40s. Once he achieved ‘FIRE status’ JACHO and hospital administration determined he was too much of a fire risk to be in the operatingroom.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. David Gaba, Steven Howard, and Sara Goldhaber-Fiebert.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” Why should anesthesiologists be any different? Let’s look at the issues. Employees of whom?
As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operatingroom emergencies. An anesthesia emergency occurs without warning.
This week the Palo Alto (California) Weekly ran a feature story on Rick Novak and Doctor Vita Uploaded: Thu, Jun 6, 2019, 9:27 am Doctor by day, sci-fi novelist by night Longtime Atherton resident spotlights AI and medicine in books by Angela Swartz / Dr. Rick Novak poses for a portrait at Stanford Hospital in Palo Alto on May 23.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. Hospital systems will have increased incentives to perform anesthetics with cheaper labor. An on-call anesthesiologist came to work at 7 a.m.,
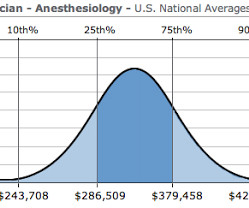
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
Almost every anesthesiologist in America has experience with surgery using the da Vinci robot system. Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? Assistant surgeon(s) and techs stand at the patient’s side, watch the surgery on video screens, and assist during the operation.
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them. Do anesthesiologists have surgeries which last 10 hours?
I’m an anesthesiologist, and I like to tell stories. I contacted the group via telephone, mailed them my resume, and they invited me to travel to their hospital for an interview. This is where the story gets more interesting, because I was not a fully trained anesthesiologist yet. We’ll be in the operatingroom with you.”
Such clinics can increase operatingroom efficiency and decrease day-of-surgery cancellations and delays, and are especially important prior to major inpatient surgeries such as brain surgeries, chest surgeries, abdominal surgeries and major transplants. Anesthesiologists need the answers to #1 and #2 above.
Dental cases are common, and are frequently referred to a hospital because the typical care systems at an outpatient surgery center or a dental office are inadequate to complete a successful anesthetic. He refuses to change into a hospital gown, or to remove his long-sleeved sweater. mg/kg midazolam, and.02
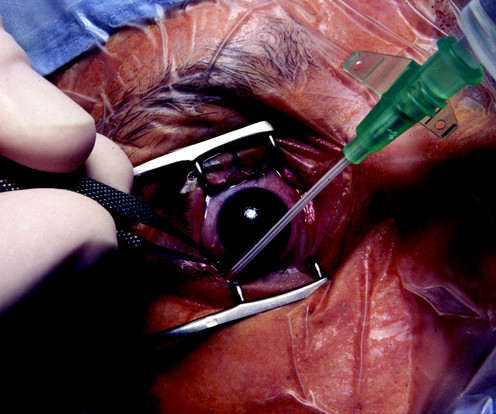
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. The second issue in this case is that you’re not a pediatric anesthesiologist. A children’s hospital or a university hospital will have a team of pediatric anesthesiologists with specialized training on call for emergencies.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. I agree with him that the current cumbersome EHRs come between doctors and patients during hospital care.
In an operatingroom, the CRNA administers the anesthesia according to the predetermined plan and monitors the patient’s vitals in order to adjust levels as needed. The CRNA is a key team member within the operatingroom and their education and experience are imperative for optimal patient outcomes.
Should you buy these books, or should you advocate that your hospital purchase them for the medical library? Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. Cote’s book has been the bible for pediatric anesthesiologists for nearly fifty years.
My friend, colleague, and President of the company I work for, the Associated Anesthesiologists Medical Group in Palo Alto, California, wrote an excellent column describing Locker Slammers for the American Society of Anesthesiologists Monitor (September 1, 2018; Volume 82, Number 9). Read on–you won’t be disappointed.
The key is finding the balance between optimizing operatingroom utilization and maintaining staff well-being. This unpredictability leads to a constantly changing schedule, which can result in either underutilized or overbooked operatingrooms.
The 2023 American Society of Anesthesiologists Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade were published last month.The paper is backed by strong science, and references an exhaustive list of no less than 277 previous publications on the topic, including this review. A 2010 survey documented that 9.4%
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Doctors and hospitals who failed to adopt a government-approved EMR system by the end of 2014 faced cutbacks in their Medicare reimbursements. hospitals have an EMR system. How can a hospital recoup this cost?
Medicare for All would decimate the specialty of physician anesthesiologists in America. The Medicare pay rate for anesthesiologists is a mere fraction of the current insurance pay rate. If a physician anesthesiologist is forced to take a pay cut to 35%-45% of their previous income, they will be upset too. of insured rates.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content