This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Evolution of Procedures and Procedural Areas Procedures that used to be hospital-based have increasingly moved into outpatient settings and physician’s offices. They estimate 4,800 anesthesia professionals left the workforce in 2022, including 2,500 anesthesiologists, 2,200 nurse anesthetists, and 65 anesthesiologist assistants.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. A doctor or a nurse?
Without a doubt, the operating room (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. So, why aren’t hospitals developing and expanding the OR? Still, with the OR a prime revenue-generator for any hospital, its operation should be scrutinized to see where cost-savings might be implemented.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. Your hospital contains multiple operating rooms, and today you are in room #10.
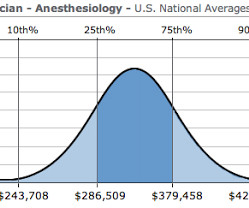
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. Hospital systems will have increased incentives to perform anesthetics with cheaper labor. An on-call anesthesiologist came to work at 7 a.m.,
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” Why should anesthesiologists be any different? Let’s look at the issues. Employees of whom?
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
This network of patients will serve to keep their clinics and hospitals full and profitable. Anesthesia providers, be they physician anesthesiologists or nurse anesthetists, are tasked with providing safe and quality anesthesia care. You may be an outstanding anesthesiologist, but you are replaceable.
During the dayshift, working alone is seldom an issue for any anesthesiologist. A typical hospital will have dozens of other anesthesia providers working in the same building. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. There are multiple different models of anesthesia care.
At an academic/university hospital, the anesthesiologist might be a resident MD in his or her first, second, or third year of anesthesia training, and that resident will then be supervised by a faculty member who is responsible for either one operating room or two. It doesn’t have to be this way. Peruse the list.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Every hospital operating room is equipped with a computer connected to the internet. Anesthesiologists type information into the EMR multiple times during each case.
When an anesthesiologist finishes their formal training, he or she has a brain full of academic teachings, and has performed hundreds of anesthetics in a university setting while being supervised by faculty members. It’s the most difficult transition in an anesthesiologist’s career. But are you ready to work alone?
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. Some anesthesiologists were initially skeptical about the ACT idea. What do you do?
THE JULY EFFECT AND THE NOVEMBER EFFECT: In American teaching hospitals, newly minted doctors begin internships each July. The term “July Effect” was coined to describe this shift change in academic hospitals each July, when the arrival of inexperienced doctors may increase the risks of medical care.
Anesthesiologists work in operating rooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. My medical board certifications are in internal medicine and anesthesiology—two fields which have significant overlap in their knowledge base but radically different practice settings.
At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation. The anesthesiologist decided to extubate the trachea at that time. Extubation is risky business. The patient began to cough.
In 2004 the Japanese Society of Anesthesiologists reported 2,443 cardiac arrests (6.34 Two other significant risk factors were emergency surgery and the patient’s preoperative health as assessed by the American Society of Anesthesiologists (ASA) physical status ranking. How common are cardiac arrests during surgery? per 10,000 cases.
These three words make any anesthesiologist cringe. The topic of anoxic encephalopathy as related to anesthesia disasters and brain death—a issue that can ruin both a patient’s life and an anesthesiologist’s career—is not specifically covered in Miller’s Anesthesia. The anesthesiologist decided to extubate the trachea.
anesthesia, I see commandments as guidelines for how to be a safe and excellent anesthesiologist. Anesthesiologists are tasked with the screening and evaluation of their patients prior to surgery , with keeping their patients safe during surgery , and with treating all medical problems immediately following the anesthetic care and surgery.
CRNAs operate safely in every setting where anesthesia is administered, including hospital operating and delivery rooms; ambulatory surgical centers; the offices of dentists, podiatrists, ophthalmologists, and plastic surgeons; pain management centers and more. " CONTACT:Kurt Knaus P: 717-724-2866 E: kurt@ceislermedia.com
How do I know if my hospital has qualified perfusionists? These highly trained professionals work closely with surgeons and anesthesiologists to maintain the patient’s circulation, regulate body temperature, and administer medications during surgery. What should I know before a procedure requiring perfusion? What is perfusion?
It was Johnny’s first day of school and my first day to report to the local hospital. I needed to be at Hibbing General Hospital before 7:30. The hospital was a three-block hike from Dom’s house, so it made sense to leave the battered BMW on the curb and walk to Hibbing General. The kitchen was quiet as a library.
The testing includes a peer-conducted clinical skills assessment by three medical staff members, a comprehensive physical exam, and cognitive screening under supervision of the neuropsychiatry department, to address the applicant’s capacity to perform the clinical privileges requested. appeared first on The anesthesia consultant.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content