This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
link] Efficient Case Scheduling - Secret to a Well-Run OR Operatingroom costs can be categorized as fixed or variable. Variable costs are largely driven by caseload and associated labor costs that occur outside of normal operational hours. Anesthesiologists, surgeons, and other clinical team members must arrive on time.
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurse anesthetists, and 3,200 anesthesiologist assistants.
The Realizing Improved Patient Care through Human-Centered Design in the OperatingRoom (RIPCHD.OR) learning lab uses a socio-technical approach incorporating human factors engineering and evidence-based design principles to create an optimal ergonomically sound operatingroom that results in improved patient and staff safety.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ Is this a watershed moment for the profession of physician anesthesiologists? Are CRNAs going to replace MD anesthesiologists all over America, changing the profession forever?
What qualities define an outstanding anesthesiologist? Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Rather, I’m choosing to list the qualities I’ve witnessed that make physician anesthesiologists stand out as leaders.
The CSFA is not just a passive participant in the operatingroom; they are an active collaborator who anticipates the surgeons needs, manages surgical instruments, and assists with critical tasks such as suturing, tissue manipulation, and hemostasis (control of bleeding). Ensuring proper wound care and dressing application.
We also had the President of the New York State Society of Anesthesiologists, Dr. Jason Lok, and Dr. John Fiadjoe, Executive Vice Chair of Anesthesia at Boston Children’s Hospital and Director of the American Board of Anesthesiology, joining us at the conference. Attendees for the annual meeting even stayed until the end on Sunday!
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. References “Anesthesia as a Career,” American Society of Anesthesiologists, March 25, 2024. Role of the Anesthesiologist.”.
Anesthesia emergencies are anxiety-producing for both experienced and inexperienced anesthesiologists, but experienced doctors are more likely to know exactly what to do and what not to do. Perioperative” means “the time around an operation”—specifically the preoperative, postoperative, and intraoperative times.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade.
At one New York medical center, intense clinical demands and provider fatigue have inspired one anesthesiologist to push the boundaries of clinical medicine. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
Will Gawande change the future for anesthesiologists? Let’s look at these three proposed Gawande changes, and how they affect the future for anesthesiologists: Taking out the trash. From the exam room to the operatingroom, doctors today follow a clear set of protocols that Dr. Gawande helped establish.
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
You utilize the current multimodal strategies for operatingroom anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% Neurosurgeons have taken him to the operatingroom to drain the hematoma and decompress the spinal column. He’s right. What happened?
Hospital surgical support encompasses a wide range of specialized services designed to assist surgeons, anesthesiologists, and nurses in performing successful surgical procedures. Prevents surgical site infections (SSIs) , a leading cause of post-operative complications. What Is Hospital Surgical Support? Why Is It Important?
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. Anesthesiologists win the tally for most operatingroom hours per week.
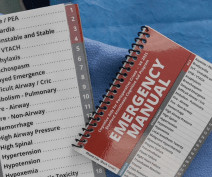
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. David Gaba, Steven Howard, and Sara Goldhaber-Fiebert.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The required parts are an operatingroom anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps. The video is posted here.
As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operatingroom emergencies. An anesthesia emergency occurs without warning.
Imagine this: I’m a brand new attending critical care anesthesiologist in a major academic medical center and in an effort to make up for the opportunity costs of becoming a doctor, I willingly take on a very aggressive clinical schedule. Setting the scene Let’s back up for a moment and set the scene.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. CRNA Only Under this model, anesthesia care is delivered by CRNAs independently, without the involvement of an anesthesiologist. So, why aren’t hospitals developing and expanding the OR?
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. You will wear a mask in the preoperative room, and that mask will remain on your face until just prior to the induction of anesthesia.
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
Peter, MN – Physician on FIRE , an anesthesiologist and financial blogger , recently hit the magical goal of Financial Independence and Retire Early (FIRE) in his mid 40s. Once he achieved ‘FIRE status’ JACHO and hospital administration determined he was too much of a fire risk to be in the operatingroom.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
Why should anesthesiologists be any different? In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurse anesthetists in multiple operatingrooms. Physician anesthesiologists pay their nurse anesthetists as employees as well as their other expenses, and then divide the profit.
Photo by Magali Gauthier/The Almanac Between his time in the operatingroom, teaching, and raising his three sons, Atherton resident Dr. Rick Novak has found time to write two novels. Rick Novak poses for a portrait at Stanford Hospital in Palo Alto on May 23.
Items 1 – 5 are discussed as follows: Non-anesthesiologists can reverse the effects of remimazolam with flumazenil if they overdose a patient, but this advantage is less important for anesthesia professionals. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent.
Such clinics can increase operatingroom efficiency and decrease day-of-surgery cancellations and delays, and are especially important prior to major inpatient surgeries such as brain surgeries, chest surgeries, abdominal surgeries and major transplants. Anesthesiologists need the answers to #1 and #2 above.
The lecture reviewed the literature regarding CICO events, and concluded that performing a surgical airway through the cricoid membrane is an essential skill for anesthesiologists. It’s essential expertise for myself and for every anesthesiologist. I’ve done thousands of cases over 34 years.
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them. Do anesthesiologists have surgeries which last 10 hours?
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. There will be a paucity of new drugs to change the practice of operatingroom anesthesia. An on-call anesthesiologist came to work at 7 a.m.,
Are anesthesiologists on the verge of being replaced by a new robot? THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Why is this robotic device only a small step toward replacing anesthesiologists?
In an operatingroom, the CRNA administers the anesthesia according to the predetermined plan and monitors the patient’s vitals in order to adjust levels as needed. The CRNA is a key team member within the operatingroom and their education and experience are imperative for optimal patient outcomes.
Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. Both surgeons and anesthesiologists analyze each procedure, and include the pertinent details of might be described as an “anesthesia recipe” for each type of case.
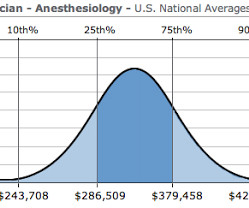
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
The key is finding the balance between optimizing operatingroom utilization and maintaining staff well-being. This unpredictability leads to a constantly changing schedule, which can result in either underutilized or overbooked operatingrooms.
One of the changes our profession has gone through is an ever-increasing demand to multitask, be it by running more than one operatingroom, or by simultaneously performing administrative or teaching tasks. Will some form of Doctor Vita populate future operatingrooms? How will we do anesthesia in the future?
Medicare for All would decimate the specialty of physician anesthesiologists in America. The Medicare pay rate for anesthesiologists is a mere fraction of the current insurance pay rate. If a physician anesthesiologist is forced to take a pay cut to 35%-45% of their previous income, they will be upset too. of insured rates.
My friend, colleague, and President of the company I work for, the Associated Anesthesiologists Medical Group in Palo Alto, California, wrote an excellent column describing Locker Slammers for the American Society of Anesthesiologists Monitor (September 1, 2018; Volume 82, Number 9). Read on–you won’t be disappointed.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content