This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
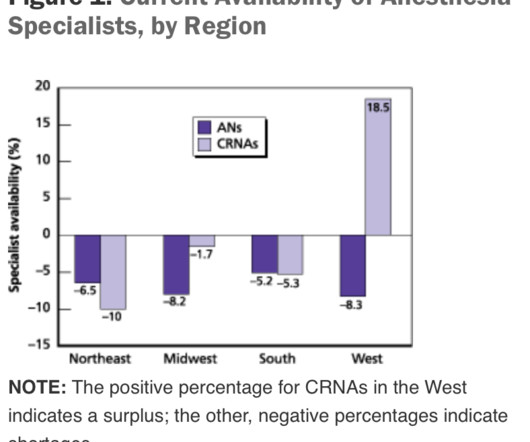
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurse anesthetists, and 3,200 anesthesiologist assistants.
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. References “Anesthesia as a Career,” American Society of Anesthesiologists, March 25, 2024. Role of the Anesthesiologist.”.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ Is this a watershed moment for the profession of physician anesthesiologists? Are CRNAs going to replace MD anesthesiologists all over America, changing the profession forever?
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. The benefits of this model are that there are fewer providers involved and less supervision needed. So, why aren’t hospitals developing and expanding the OR?
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Every hospital operatingroom is equipped with a computer connected to the internet.
During the dayshift, working alone is seldom an issue for any anesthesiologist. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. Unlike Alex Honnold, the anesthesiologist is not putting their own life at risk—rather it is their patient who is at risk. Working alone may be less safe.
Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. A board-certified physician anesthesiologist is therefore validated as an expert in all areas of perioperative medicine. Most anesthetics are conducted by physician anesthesiologists. Are CRNAs and anesthesiologists equals?
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operatingroom. Anesthesiologists in our practice telephone their patients the night before to discuss the anesthesia care.
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. A team led by an attending anesthesiologist uses remote monitoring to provide evidence-based support to anesthesia colleagues in all the operatingrooms.
Why should anesthesiologists be any different? In many private practice anesthesia groups, physician anesthesiologistssupervise multiple nurse anesthetists in multiple operatingrooms. Physician anesthesiologists pay their nurse anesthetists as employees as well as their other expenses, and then divide the profit.
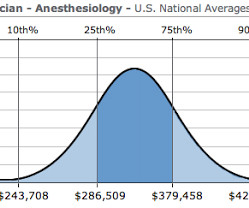
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
Instead of writing histories, examining patients, making diagnoses, and prescribing medications as interns and internal medicine doctors do, anesthesia residents are rendering their patients unconscious, applying acute pharmacology, and inserting tubes and needles into patients in operatingrooms at all hours of the day and night.
In the operatingrooms, the patients are brought in by the surgeons. Anesthesia providers, be they physician anesthesiologists or nurse anesthetists, are tasked with providing safe and quality anesthesia care. Note that anesthesiologists who specialize in pain medicine in a clinic setting can be exceptions to this discussion.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. There will be a paucity of new drugs to change the practice of operatingroom anesthesia. An on-call anesthesiologist came to work at 7 a.m.,
In 2004 the Japanese Society of Anesthesiologists reported 2,443 cardiac arrests (6.34 Two other significant risk factors were emergency surgery and the patient’s preoperative health as assessed by the American Society of Anesthesiologists (ASA) physical status ranking. Anesthesiologists will continue to be challenged.
One of the changes our profession has gone through is an ever-increasing demand to multitask, be it by running more than one operatingroom, or by simultaneously performing administrative or teaching tasks. It is 2030 and I am scheduled to supervise anesthesia for a 40-yr-old patient undergoing laparoscopic cholecystectomy.
Between them, Larson and Jaffe have supervised tens of thousands of anesthetics in a university practice. Now, because of this book, readers can find on the printed page what the authors taught in the preoperative forum, in the operatingroom, and in the post-anesthesia recovery room. Together, Drs.
At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation. The anesthesiologist decided to extubate the trachea at that time. Extubation is risky business. The patient began to cough.
Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operatingrooms/intensive care units. Let’s look at each of these in turn.
These three words make any anesthesiologist cringe. The topic of anoxic encephalopathy as related to anesthesia disasters and brain death—a issue that can ruin both a patient’s life and an anesthesiologist’s career—is not specifically covered in Miller’s Anesthesia. The anesthesiologist decided to extubate the trachea.
I entered the hallway of the operatingroom complex. Hibbing General had only six operatingrooms, compared to the 40 rooms at Stanford. My old med school classmate, Michael Perpich, the Chief of Staff at Hibbing General, was the surgeon working in operatingroom #1. Nice to meet you,” I said.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content