This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered NurseAnesthetist (CRNA) is a journey marked by immense growth but also profound challenges. ICU nurses are adept at managing complex critical care situations, which provides a solid foundation for a career in anesthesia.
What’s the difference between a physician anesthesiologist and a nurseanesthetist? There is no fork in the career path that makes a busy Certified Registered NurseAnesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. The answer: internal medicine. In a way, it is.
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. To begin, it’s essential to understand the role of a CRNA. CRNAs received specialized training that is critical in surgeries and healthcare.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. Non-emergency surgery may be delayed for days, weeks, or longer. Consolidation of surgery locations from understaffed rural facilities to urban/suburban hospitals and surgery centers is likely.
Advanced Practice Provider Spotlight: Certified registered nurseanesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurseanesthetist (CRNA) at Penn State Health Milton S.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). Are CRNAs and anesthesiologists equals?
Who is responsible for your safety before, during, and after your surgery? Will it be a nurse or will it be a physician? The word “perioperative” means “around the time of surgery.” It’s officially defined as the 30-day time period following surgery. Note this data was for inpatient surgeries. No, they are not.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The anesthesiologist meets the patient prior to the surgery, reviews the chart, and examines the patient.
Their education, training and expertise is impressive and very appreciated by our surgical centers, CRNA s and patients. An anesthesiologist is a medical doctor who plays a critical role in the preparation, execution, and recovery stages of surgery. Salem Anesthesia is fortunate to have the best Anesthesiologists on our team.
Ashley Bell, BSN, RN , has always been fascinated by the way patients are put into a state where they are unable to feel and respond to outside stimuli, and then when they awake, they have no recollection of what took place throughout the surgery.
While few administrators would consider reducing the number of surgeries (that would strangle the golden goose!) All MD In this model, (most prevalent in one-or two-room surgery centers and less common in large ambulatory surgery centers), all anesthesia care is provided by medical doctors only, specifically physician anesthesiologists.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The University of Michigan paper stated, “this study primarily analyzed physician-CRNA teams, the dominant practice model in US anesthesiology.” million charts were studied.
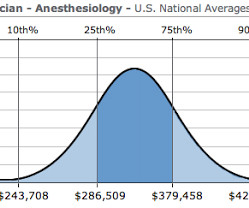
The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list. The median salary of nurseanesthetists was listed as $160,270, and the unemployment rate as 2.7%. Expect the demand for acceptance into physician anesthesiologist and nurseanesthetist training programs to remain high.
It’s not clear the idea has widespread traction as of yet, and the concept will always be at odds with the individual aspirations of internal medicine doctors, hospitalists, intensivists, surgeons, and certified nurseanesthetists, all who want to make their own management decisions, and all who desire to be paid for owning those decisions.
The good news for the future of anesthesia careers is that the number of surgeries in the United States is expected at increase as the Baby Boomers age. One model is having a CRNA do the anesthetic independently without any physician anesthesiologist present. The demand for anesthesia services will grow.
These devices enable an anesthesiologist to remain connected to the outside world during surgery. A patient’s EMR combines information from previous clinic visits, emergency room visits, laboratory and test results, and all data from the preoperative, intraoperative, and postoperative course on the day of surgery.
NurseAnesthetist If you’re looking for a lucrative career and are prepared to invest time and effort in advanced training, consider becoming a Certified Registered NurseAnesthetist (CRNA). According to the Bureau of Labor Statistics, nurseanesthetists make an average of $200,000 a year.
For healthy patients undergoing elective surgery the anesthetic risks are minimal, and are similar to the risks of driving on a freeway in an automobile. In an anesthesia care team, a physician anesthesiologist supervises up to four operating rooms and each operating room is staffed with a certified registered nurseanesthetist (CRNA).
It’s true that surgeons bring the patients to the operating room for surgery. Maybe you’re worried that nurseanesthetists will take your job away. It’s likely that simple cases such as cataracts, lymph node biopsies, and knee arthroscopies can be safely done with CRNA anesthesia. Surgeons know how to wield a scalpel.
Propofol administration requires an experienced clinician, e.g. either an anesthesiologist, a certified registered nurseanesthetist (CRNA), or an emergency medicine physician. Our chairman lectured to us, “Do you know many patients are nervous prior to their anesthesia and surgery? Every one of them.
After a surgery is finished, anesthetic gases and intravenous anesthesia drugs are discontinued, and the patient wakes up within 5 to 15 minutes. The surgery concluded 2 hours later and the anesthetics were discontinued. An 80-year-old female presented for elective right elbow surgery. Five minutes later she opened her eyes.
What sort of preoperative tests or therapies should this patient have before surgery? CHATGPT: For an 80-year-old woman with congestive heart failure (CHF) who needs to undergo gallbladder removal surgery, it is essential to conduct a thorough preoperative evaluation to assess her overall health status and identify any potential risks.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. The surgery will take approximately three hours. You’ll be asleep for the entire surgery.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. A 40-year-old male presented for outpatient septoplasty surgery. The surgery concluded 4 hours later.
Anesthesiologists in training, practicing anesthesiologists, and Certified Registered NurseAnesthetists (CRNAs) must receive hands-on education on performing front of neck access, as well as the reasoning behind not delaying the procedure. You’re an anesthesiologist or a CRNA. Evaluate each airway prior to surgery.
by PennLive.com Patients undergoing surgery or procedures requiring anesthesia are safe when cared for by a physician anesthesiologist, a certified registered nurseanesthetist (CRNA), or both. 3) relates to outdated and restrictive laws that prevent CRNAs from practicing to their fullest scope. Published: Jan.
The faded turquoise tile on the walls had witnessed thousands of hernia surgeries. The nurseanesthetist ignored Perpich’s cordial introduction and said nothing to me. He was only a nurseanesthetist. We have six nurseanesthetists, but for tough cases we need an M.D. Six nurseanesthetists.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content