This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. Command centers will likely allow professionals to supervise an increased number of locations safely in the operatingroom. Imagine this: It’s the year 2034. Leverage technology.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. The benefits of this model are that there are fewer providers involved and less supervision needed. So, why aren’t hospitals developing and expanding the OR?
If a CRNA presents themselves as the sole anesthesia professional responsible for evaluating you and making the anesthesia plan and carrying out all the anesthesia care, you realize you’re not being attended to by a physician. Physician anesthesiologists frequently employ CRNAs to assist them in the anesthesia care team model.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Every hospital operatingroom is equipped with a computer connected to the internet. Love it or hate it, the EMR is here to stay.
Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. In this model, an MD anesthesiologist supervises up to four CRNAs who work in up to four different operatingrooms simultaneously. Are CRNAs and anesthesiologists equals? Why do patients die?
In an anesthesia care team, a physician anesthesiologist supervises up to four operatingrooms and each operatingroom is staffed with a certified registered nurse anesthetist (CRNA). In many hospital operatingrooms, a solitary physician anesthesiologist attends to his or her patient alone.
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operatingroom. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10. Then we’ll roll down the hallway into the operatingroom. and to bring your cell phone with you.
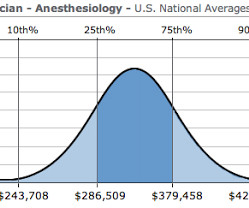
An operatingroom anesthesia practice is somewhat akin to being a taxi cab driver. One model is having a CRNA do the anesthetic independently without any physician anesthesiologist present. So a critical first question to ask is if the big three benefits are/are not part of the promised salary.
In contrast, other operatingroom professionals are usually relaxed and winding down at this time, because the surgical procedure is finished. Will your anesthesia professional be a physician anesthesiologist, a Certified Registered Nurse Anesthetist (CRNA), or an anesthesia care team made up of both?
Have the Stanford Emergency Manual 5 in your operatingroom suite, and ask a registered nurse to recite the Cognitive Aid Checklist for HYPOXEMIA to you, to make sure you haven’t missed something. If an anesthesia care team is attending to you, how many rooms is each physician anesthesiologist supervising?
I entered the hallway of the operatingroom complex. Hibbing General had only six operatingrooms, compared to the 40 rooms at Stanford. My old med school classmate, Michael Perpich, the Chief of Staff at Hibbing General, was the surgeon working in operatingroom #1. The man said, “She did.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content