This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? I tried it on several of my patients who had prolonged awakening after generalanesthesia.
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Potent inhalation anesthesia (sevoflurane). What do you do?
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). She walked out of the hospital two days later.
Anesthesiavitalsigns monitor display A second and more compelling use for smart glasses would be the display of a patient’s vitalsign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vitalsign electronic monitors.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. This is every anesthesia provider’s nightmare. Four liters/min of oxygen are administered intranasally.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. Your hospital contains multiple operating rooms, and today you are in room #10.
Vigilance regarding a sleeping patient’s vitalsigns was always paramount, but the constant effort to be vigilant could be mind-numbing. Since the development of the internet, anesthesia practice has changed forever. Every hospital operating room is equipped with a computer connected to the internet.
Miller’s Anesthesia , 9 th edition, Chapter 31, Preoperative Evaluation) All adults and adolescents should be questioned regarding their history of alcohol use prior to anesthesia. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia? cannabis REF) are present.
On physical exam, her vitalsigns are normal, her lungs are clear, and her heart exam is positive for the clicking sound of a mechanical valve and a 2/6 systolic murmur. Vitalsigns remain normal with BP=110/70, P=80, and oxygen saturation=99%. She is obese, weighing 200 pounds, with a BMI=35. She is on no medications.
How can it be that generalanesthesia has ceased to evolve? What about monitors of vitalsigns? The standard monitoring devices of pulse oximetry, end-tidal CO2 monitoring, and other essential anesthesiavitalsign monitors were developed and in use by the 1990s.
Maggie is paralyzed from the neck down— a ventilator-dependent quadriplegic—and is hospitalized in a private room. Then he injects her IV with a syringe of adrenaline, and leaves the vitalsigns monitor on. The vitalsigns monitor shows her heart rate suddenly change to zero as she dies. Remarkable! Coma (1978).
Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operating room 13 of Stanford University Hospital. Upon arrival at the airport in the donor city, an ambulance transported us to the hospital.
The physical exam includes the height, weight, vitalsigns, and documentation of any abnormal findings on exam of the entire body. Plan: cleared for generalanesthesia providing ECG and labs are normal. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia?
An anesthesia machine, with the vitalsigns monitor screen on the left, and the electronic medical records computer screen on the right. His vitalsigns are heart rate = 100, BP = 150/80, respiratory rate = 20 breaths/minute, oxygen saturation 95% on room air, and temperature 100.2 The BP is 100/50.
When a Code Blue or a dire change in vitalsigns occurs in an operating room, the Manual directs the resuscitation team to the correct order of action at a time when minds are racing, thoughts have become jumbled, and near-perfect intervention is required. Why Did Take Me So Long To Wake From GeneralAnesthesia?
With influenza illness may range from mild to severe and even death, but hospitalization and death occur mainly among high risk groups such as elderly patients or those with preexisting chronic illnesses. That is the real scare of the coronavirus issue—the fear that our hospitals could not handle the volume of severe infections.
An anesthesia emergency occurs without warning. Your patient’s vitalsigns are dropping. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group.
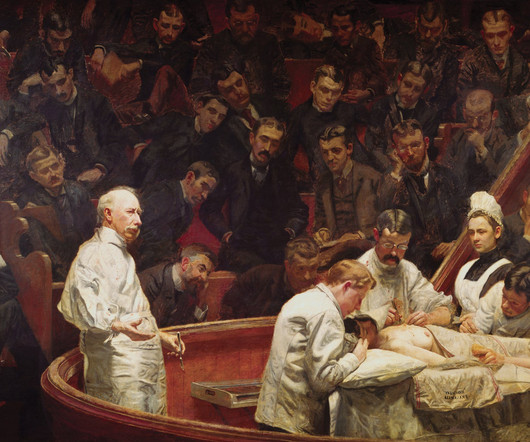
The first public demonstration of anesthesia, at the Ether Dome in Massachusetts GeneralHospital Important advances in the history of anesthesia changed medicine forever. Humans have inhabited the Earth for 200,000 years, yet the discovery of surgical anesthesia was a relatively recent development in the mid-1800s.
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT).
In July 1984 during the first week of my Stanford anesthesia residency at the Santa Clara County Hospital, the entire medical center owned only three Nellcor pulse oximeters. The oxygen saturation became recognized as “the fifth vitalsign,” joining heart rate, blood pressure, respiratory rate, and temperature.
How soon will we see robotic anesthesia in our hospitals and surgery centers? Most of these discoveries originated in Silicon Valley, just miles outside Stanford University Hospital where I’ve been working for the past 42 years. Our medical world inside the hospital has changed more slowly. Relatively little.
Tell the surgeon that the patient needs to have cardiac clearance prior to any general anesthetic, and that the case needs to be done in a hospital setting rather than at a freestanding surgery center. Just do MAC (Monitored Anesthesia Care) anesthesia for this case, but make sure he’s asleep.
His hospital chart shows no past anesthetics, and he has no medical problems except hypertension which is treated with lisinopril. His vitalsigns are normal, and his oxygen saturation is 96% on room air.You are six months out of anesthesia training and new to this hospital. What went wrong here?
“Free-soloing” describes the most anxiety–producing event in every anesthesiologist’s life: the transition from anesthesia training when your faculty member is backing up your every move and every mistake, to the real world of anesthesia when you have to do scary cases alone without assistance. at a community hospital.
An ICU physician will write an order for the dosing of intravenous fentanyl, and the ICU nurse will be in constant attendance to monitor the patient’s vitalsigns and level of sedation. After surgery, hospital inpatients who have postoperative pain are typically treated with longer acting narcotics such as morphine or Dilaudid.
Be wary when administering generalanesthesia to any patient who cannot walk up two flights of stairs. This requires preoperative workup to determine the diagnosis and to apply treatment prior to generalanesthesia. I refused to staff the case, and told him, “Cases like this—that’s why we have hospitals.”
INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under generalanesthesia. Current electronic medical records (EMR) systems exist in every hospital, and the EMRs are generating the sort of Big Data that algorithms will be built on.
The procedure does not require a breathing tube, so we’ll administer the sedation and be vigilant regarding what happens to the patient’s vitalsigns. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
AI computers will be stocked with information from multiple sources, including all known medical knowledge published in textbooks and journals, as well as the electronic health records (EHR)/ clinical data from thousands of previous hospital and clinic patients. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Imagine you’re two months out of anesthesia training, working at a community hospital, and at 2 a.m. you need to induce emergency anesthesia for a 300-pound man who just ate a full meal of pizza and beer two hours earlier. You’re working alone without that anesthesia attending who stood next to you during residency training.
Neither ciprofol nor propofol caused statistically significant differences in vitalsigns. 2022) conducted a phase III study at ten teaching hospitals, comparing ciprofol and propofol for deep sedation for colonoscopy or gastroscopy. mg/kg for the induction of generalanesthesia. Chen et al. Wang et al.
His preoperative vitalsigns were normal with an oxygen saturation of 98%. Anesthesia was induced with propofol 250 mg, fentanyl 100 micrograms, and rocuronium 50 mg IV. His preoperative vitalsigns were normal. He walked out the hospital alive and well. Will I Have a Breathing Tube During Anesthesia?
Prior to surgery your patient tells you, “I always get a hangover after generalanesthesia. Hangover after generalanesthesia (HAGA) describes a patient who has a safe general anesthetic, but who then feels hungover, sedated, and wasted for a time period exceeding two hours afterwards. The patient is always right.
All four reach the surface, alive and anesthetized, and are transported to a nearby hospital. Anesthetized patients have no muscle movement and are unable to generate any body heat in the cold water. No one monitored the vitalsigns of the boys during their 3-hour underwater general anesthetics.
In the 1990s we were documenting all anesthesia care with pen on paper. Today hospitalanesthesia medical records are recorded into computer software. Another study published in JAMA found that private equity-backed hospitals may have worse quality of inpatient care. Hospital subsidies for anesthesia groups.
You learn to inject propofol and intubate a patient in the first few months, but its a lifetime journey to master the medical aspects of evaluating and treating the heart, lungs, brain, kidneys and vitalsigns during anesthesia care. The goal is to be a perioperative (around the time of operation) doctor, not a technician.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content