This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Does exposure to generalanesthesia cause dementia? Association of Mild Cognitive Impairment With Exposure to GeneralAnesthesia for Surgical and Nonsurgical Procedures: A Population-Based Study. All of their anesthesia records for surgeries after the age of 40 were reviewed. In a word, “No.” Anesthesiology.
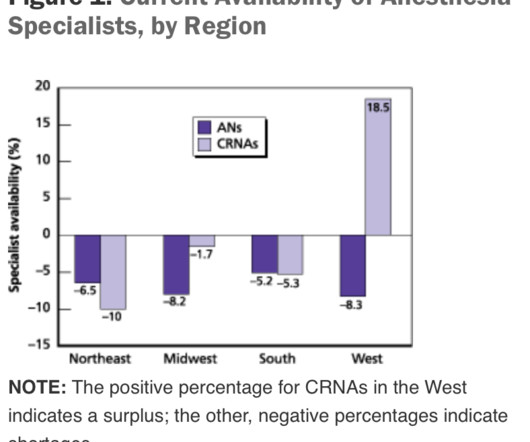
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population). of the population).
When the general anesthetic requires an endotracheal tube, an issue is how to awaken the patient with minimal patient coughing and bucking while the tube remains in the trachea. An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. to 25 μg/kg/hr.” “We
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation.
preparing to remove an endotracheal tube from a patient Every general anesthetic has risk. The conclusion of most general anesthetics requires the removal of a breathing tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. In the immortal words of Forrest Gump, “Sh*t happens.”
But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. No, it’s not the nurseanesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies.
Will it be a nurse or will it be a physician? A 2013 study in Anesthesiology states, “Despite the fact that a surgical procedure may have been performed for the appropriate indication and in a technically perfect manner, patients are threatened by perioperative organ injury. This is an important question. Why do patients die?
I work in a private practice setting in Palo Alto, California, and liposuction is one of the most common plastic surgery procedures performed. Early in my career, in the late 1980’s, liposuction was a bloody procedure. Preanesthetic assessment and patient selection are key for safe large-volume liposuction procedures.
The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. Patients with autism commonly need to be sedated for routine procedures that a normal child or adult would cooperate with. The mother was adamant that the procedure needed to be performed.
Food and Drug Administration (FDA) is warning that repeated or lengthy use of general anesthetic and sedation drugs during surgeries or procedures in children younger than 3 years or in pregnant women during their third trimester may affect the development of children’s brains. The answer to all these questions is: “It depends.”
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The trachea is intubated, and anesthesia is maintained with 1-1.5% The surgery concludes at 1630 hours.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. I’m writing this in January 2016.
Regional anesthesia is a growing frontier in modern clinical anesthesia, in part because of the availability of ultrasonic imaging to help us direct needle placement. The subspecialty of regional anesthesia has blossomed. following generalanesthesia in contrast to a peripheral nerve injury rate of 1.7%
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. binocular Moverio BT-35E smart glasses A South Korean group led by Dr. Y.E.
Control of the airway is the most important clinical priority in anesthesia care. The INTUBATION AFTER INDUCTION OF GENERALANESTHESIA section of the Difficult Airway Algorithm is bifurcated into two pathways. The most critical technical skill for an anesthesiologist is. facemask ventilation.
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient. Every anesthesia provider carries a smartphone connected to the internet. Many anesthesia providers carry a laptop or a tablet in their briefcases. Love it or hate it, the EMR is here to stay.
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
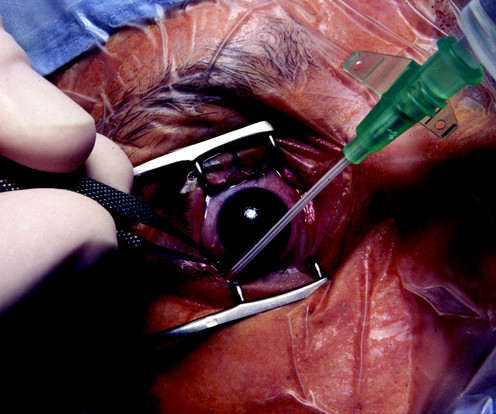
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. A 3-year-old boy is eating a McDonalds Happy Meal on the lawn of the restaurant.
The safety of anesthesia on ASA I and II patients has been compared to the safety record of commercial aviation. A total of 266 cases of brain damage or death during anesthesia care in the operating room under the care of a solo anesthesiologist occurred. But planes do crash, and so do anesthetized patients.
The surgical attendings were the kings, the students were the peasants, the nurses and techs were serfs, and the anesthesiologists were the whipping boys for the surgeons. Some people have difficulty seeing the outstanding merits of physician anesthesiology. I understand where these opinions come from, but the phenomenon still bothers me.
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 A surgical airway is an invasive airway via the front of the patient’s neck into their trachea.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. You leave your street clothes in your locker.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. Medications may need to be adjusted or temporarily stopped to minimize potential risks during the procedure. This could indicate a cardiac event or a complication related to the anesthesia.
The procedure was to be done in the prone position, and required endotracheal intubation. The patient was turned prone, and the procedure commenced. After only 15 minutes of operating time, the gastroenterologist announced that the procedure was over. The trachea was extubated. The nadir oxygen saturation was 49%.
We’re going to sedate this patient for a medical procedure. The procedure does not require a breathing tube, so we’ll administer the sedation and be vigilant regarding what happens to the patient’s vital signs. Let’s discuss a hypothetical male patient. He is 79 years old, overweight, and has a thick neck.
Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operating room 13 of Stanford University Hospital. Note that the anesthesia transport team member was only an anesthesia fellow or a resident.
These alarms would bring a fleet of nurses and/or doctors into the room to try to save the patient. I love the movies, but it can be painful to watch scenes where the facts are distorted, sometimes so much that the storyline is implausible. This film is my Hollywood medical pet peeve, and the movie that motivated me to write this column.
I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Learn to perform medical procedures at the highest level.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. I’m fascinated by the topic of artificial intelligence in medicine. This is the third column in a series regarding robots in medicine. Smartphones verbally direct us to our destination through mazes of highways and traffic.
Instead of writing histories, examining patients, making diagnoses, and prescribing medications as interns and internal medicine doctors do, anesthesia residents are rendering their patients unconscious, applying acute pharmacology, and inserting tubes and needles into patients in operating rooms at all hours of the day and night.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
How do you feel when you meet your anesthesia provider prior to a surgical procedure? In an abstract presented at the 2015 American Society of Anesthesiologists annual meeting, data from the 2014 National Anesthesia Clinical Outcomes Registry was compiled for every anesthesiologist of known age who performed at least 100 cases.
Under anesthesia these reflexes are absent. These fasting guidelines do not apply to surgical procedures under local anesthesia, or to those with no anesthesia. The guidelines do apply for colonoscopies or upper gastrointestinal endoscopy procedures. You don’t have to fast for a dentist office visit, for example.
My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. What happens if every anesthesia patient pays only Medicare rates in a Medicare for All future? 75 X $76) + (.25
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content