This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population). of the population).
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. binocular Moverio BT-35E smart glasses A South Korean group led by Dr. Y.E.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
A recent 2024 publication in JAMA looked at 8429 surgical procedures from March 2021 to December 2022 in a single institution. The anesthesiologist could indirectly visualize the patient’s vocal cords, which enabled the placement of the endotracheal tube into the windpipe. I utilize VL for difficult airway cases or emergency cases.
You take the elevator to the third floor and proceed to the locker room. The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. The Anesthesia Consultant’s 2022 List of the Top Anesthesia Books includes: Miller’s Anesthesia , 9th edition, 2019, Editor-in-Chief Michael Gropper.
The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. Patients with autism commonly need to be sedated for routine procedures that a normal child or adult would cooperate with. The mother was adamant that the procedure needed to be performed.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. An important question for many Americans is, “Is it safe for me to have surgery during this COVID pandemic?” It depends. Everyone in the healthcare facility will be wearing masks.
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct generalanesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
Allow more procedures to be performed When surgery times are shortened, surgeons and other surgery providers are able to work with more patients per day. This means that more procedures are performed, and more patients are assisted overall. However, the number of surgeries performed depends on surgery length.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. Between them, Larson and Jaffe have taught hundreds of anesthesia residents the finer points of clinical care. Philip Larson and Richard Jaffe. He was my neuroanesthesia professor at Stanford.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
Shortly after, the spinal anesthetic wore off and the patient was quickly placed under generalanesthesia. The procedure was completed uneventfully after the surgeon, Dr. Annuloplasty, unscrubbed to sucker punch Dr. Millerstein. Dr. Annuloplasty remains in a ketamine-induced haze in the corner of the operatingroom.
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
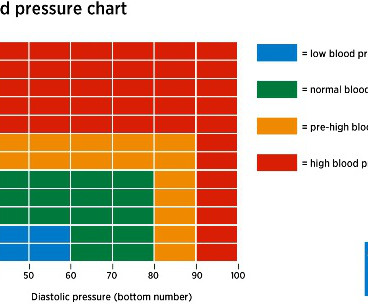
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
SCALPEL, BOUGIE, TUBE APPROACH TO CRICOTHYROIDOTOMY This week I attended an outstanding Stanford Anesthesia Grand Rounds delivered by Drs. The specter that someday we will induce and paralyze a morbidly obese patient, and then be unable to intubate or oxygenate that patient, is in the back of the mind of every anesthesia professional.
The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site. Assistant surgeon(s) and techs stand at the patient’s side, watch the surgery on video screens, and assist during the operation.
Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. There will be a paucity of new drugs to change the practice of operatingroomanesthesia.
I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Learn to perform medical procedures at the highest level.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% What do you do?
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. The surgery was done in a small community hospital where there was no ICU, blood bank, or emergency room.
Let’s discuss an elephant in the room of operatingroomanesthesia–the association between peripheral nerve blocks and nerve injury. The use of peripheral nerve blocks has crescendoed in anesthesia practice, stimulated by the use of ultrasound-guided visualization of nerves. Liu SS, et al. Why is this?
This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals. From the exam room to the operatingroom, doctors today follow a clear set of protocols that Dr. Gawande helped establish. Pearl writes, “ It’s estimated that 25 percent of all U.S.
My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. What happens if every anesthesia patient pays only Medicare rates in a Medicare for All future? 75 X $76) + (.25
Physicians see EPIC as a software system designed to make billing efficient for the hospitals, so that the hospitals can capture a charge for every dose of medication and every procedure. Want to know how to make a billion dollars in healthcare and change the world for the better at the same time? The strategy worked. The strategy worked.
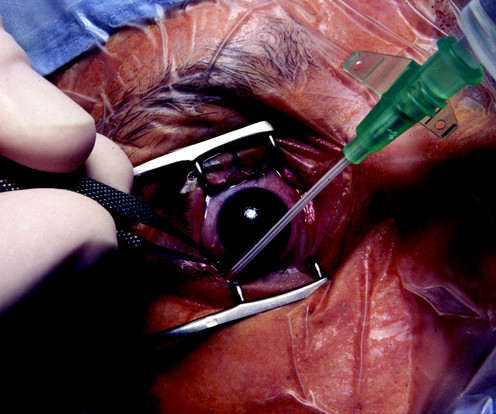
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. A 3-year-old boy is eating a McDonalds Happy Meal on the lawn of the restaurant.
The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Are anesthesiologists on the verge of being replaced by a new robot? In a word, “No.”
Pursue a career as a clinic doctor if you enjoy sitting in a room, listening to patients and talking to patients. Most clinic doctors work daytime hours, but have weekend call and night call, which may include phone consultations or emergency room visits. The sooner you understand these two forks in the road, the better off you’ll be.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? I tried it on several of my patients who had prolonged awakening after generalanesthesia.
Just before the start of anesthesia, a patient may hear the operatingroom nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
Picture this: your job requires you to spend the majority of your day in a windowless room with four other people. You cannot leave the room, and if you make a serious error in your work, someone can die. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. This may occur via a telephone call one day prior to surgery, or in the preanesthetic room on the day of surgery. Most of the time an anesthesiologist works in the operatingroom.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents.
preparing to remove an endotracheal tube from a patient Every general anesthetic has risk. The conclusion of most general anesthetics requires the removal of a breathing tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. In the immortal words of Forrest Gump, “Sh*t happens.”
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. What do you do?
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation.
I work in a private practice setting in Palo Alto, California, and liposuction is one of the most common plastic surgery procedures performed. Early in my career, in the late 1980’s, liposuction was a bloody procedure. Preanesthetic assessment and patient selection are key for safe large-volume liposuction procedures.
You’ve graduated from a residency program in which you learned the nuances of preoperative, intraoperative, and postoperative anesthesia practice. You believe the patient is high risk in terms of his airway, his breathing, his cardiac status, and his potential for post-operative complications. You’re a board-certified anesthesiologist.
The capacity to deliver this much oxygen to a non-intubated patient is a marked advance in anesthesia care. Dr. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operatingroom. At the 2023 American Society of Anesthesiologists meeting in San Francisco, I walked by a booth advertising High Flow Nasal Oxygen.
Patients assigned to continuous finger-cuff monitoring received more than twice as much norepinephrine both within 15 minutes after starting induction of anesthesia and during the entire surgery, when compared with patients assigned to intermittent oscillometric monitoring.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. I’m fascinated by the topic of artificial intelligence in medicine.
I don’t tout myself as an expert in AI technology, but I am an expert in taking care of patients, which I’ve done in clinics, operatingrooms, intensive care units, and emergency rooms at Stanford and in Silicon Valley for over 30 years. AI is already prevalent in our daily life. AI is already prevalent in our daily life.
In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. The ICU attendings had respectful peer relationships with all the surgeons, including the private-practice cardiac surgeons whose post-operative patients were housed in the ICU.
You’ve found The Anesthesia Consultant website, so you have some interest in anesthesia. The truth is: a career in anesthesia involves unique demands that most people would not seek, tolerate, or ever grow accustomed to. An operatingroom emergency is not a time for screaming, temper tantrums, or freezing.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content