This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
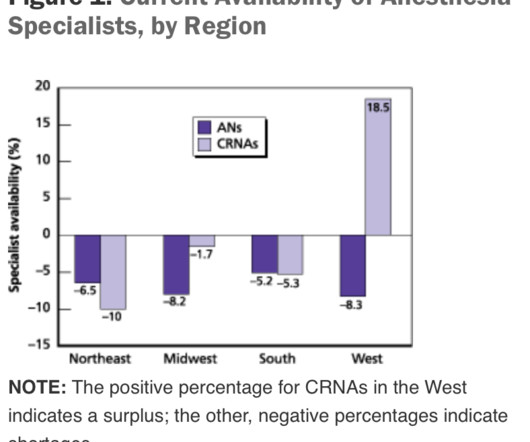
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population). of the population).
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. Between them, Larson and Jaffe have supervised tens of thousands of anesthetics in a university practice. Imagine if Yoda and Obi-Wan Kenobi wrote a book called, “The Art of Jedi Practice.”
Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. There will be a paucity of new drugs to change the practice of operating room anesthesia.
Surgeons have been using trocars for generations to minimize the trauma of surgical procedures and reduce the need for anesthesia, and to help patients recover faster. The pellets produce a baseline for testosterone that can be adjusted with occasional use of patches or injections under medical supervision.
The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. You leave your street clothes in your locker.
preparing to remove an endotracheal tube from a patient Every general anesthetic has risk. The conclusion of most general anesthetics requires the removal of a breathing tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. In the immortal words of Forrest Gump, “Sh*t happens.”
Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient. Every anesthesia provider carries a smartphone connected to the internet. Many anesthesia providers carry a laptop or a tablet in their briefcases. Love it or hate it, the EMR is here to stay.
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. I’m fascinated by the topic of artificial intelligence in medicine. This is the third column in a series regarding robots in medicine. Smartphones verbally direct us to our destination through mazes of highways and traffic.
But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. Anesthesia providers, be they physician anesthesiologists or nurse anesthetists, are tasked with providing safe and quality anesthesia care. What is this threat? What is anesthesiology’s Achilles’ heel?
A 2013 study in Anesthesiology states, “Despite the fact that a surgical procedure may have been performed for the appropriate indication and in a technically perfect manner, patients are threatened by perioperative organ injury. All the responsibility in the ACT model resides with the supervising MD anesthesiologist.
Instead of writing histories, examining patients, making diagnoses, and prescribing medications as interns and internal medicine doctors do, anesthesia residents are rendering their patients unconscious, applying acute pharmacology, and inserting tubes and needles into patients in operating rooms at all hours of the day and night.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
anesthesia, I see commandments as guidelines for how to be a safe and excellent anesthesiologist. Based on forty years of clinical practice and administration in both community and academic anesthesiology, here are Ten Commandments of Anesthesia as I see them: Be a doctor, not a propofol technician.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content