This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What’s the difference between a physician anesthesiologist and a nurse anesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurse anesthetist? The answer: internal medicine.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The PACU nurse’s name is Gloria, and she is new to this surgical facility.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesiacare unit (PACU). It’s common for zero monitoring equipment to be attached to the patient.
No one wants a partner who repeatedly creates conflict in the workplace, who initiates conflict with a surgeon in the operating room, a nurse in the postanesthesiacare unit, or an administrator. To gain a better anesthesia job, get the three A’s of ability/affability/availability aligned per the suggestions above.
He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. The surgery proceeded as scheduled, with sevoflurane as maintenance anesthesia. At the conclusion of surgery, the patient was extubated awake and taken to the PostAnesthesiaCare Unit (PACU) in stable condition.
When you enter the healthcare facility, a nurse will question you regarding virus symptoms, and will screen you by taking your temperature. The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operating room.
The patient will probably already have an IV in their arm, placed by a registered nurse. (To We do this because we’re skilled at placing IVs painlessly and successfully, it doesn’t take that much time, and it gives the patient confidence that we’ll continue to take care of them at the highest level.) sevoflurane gas to the patient.
Her breathing tube had been removed, but she developed upper airway obstruction in the PostAnesthesiaCare Unit (PACU) and needed urgent reintubation. The patient had multiple low-normal blood pressure readings over the first 5 hours postoperatively, and was being observed by the nursing staff.
You have to get along well with surgeons, the nursing staff, the scrub techs, administrators, and the patients. Their patients are obtunded on arrival to the PostAnesthesiaCare Unit (PACU) after surgery, and they rely on the PACU nursing staff to complete the job of anesthesia wake up. Some are not.
Ideally the involved MDs and nurses will fill out an Incident Report or an Adverse Event Report, which includes the details of what happened to their patient. Some reports reveal only minor issues such as prolonged post-operative nausea and vomiting, or a prolonged PostAnesthesiaCare Unit stay.
I stay with the child until the anesthetic depth has dissipated, the breathing tube is removed, and the child is awake and safe with the recovery room nurse in the PostAnesthesiaCare Unit. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
Sugammadex reversal can make the duration of a rocuronium motor block almost as short acting as a succinylcholine motor block, and sugammadex can also eliminate complications in the PostAnesthesiaCare Unit due to residual postoperative muscle paralysis. Why Did Take Me So Long To Wake From GeneralAnesthesia?
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% The patient does well, and is discharged from the PostAnesthesiaCare Unit in excellent condition.
Washington University has expanded the ACT to include the Recovery Control Tower, which provides similar surveillance over patients in the PostAnesthesiaCare Unit (PACU). This photograph below depicts the Anesthesia Control Tower manpower at work at Barnes Jewish Hospital at Washington University in St.
The surgery and anesthesia proceed uneventfully. The patient is awakened from generalanesthesia and taken to the PostAnesthesiaCare Unit. Abdominal surgery and generalanesthesia in this patient population are not without risk, even with optimal anesthetic care.
A performs a rapid sequence induction of anesthesia by injecting propofol (a hypnotic sleep drug) and succinylcholine (a muscle paralyzing drug) into the IV. The operating room nurse presses down on Mr. Doe’s cricoid cartilage in his neck, to compress the esophagus and prevent any stomach contents from regurgitating upward into the airway.
Prior to surgery your patient tells you, “I always get a hangover after generalanesthesia. Listen to them and adjust your care. Hangover after generalanesthesia (HAGA) describes a patient who has a safe general anesthetic, but who then feels hungover, sedated, and wasted for a time period exceeding two hours afterwards.
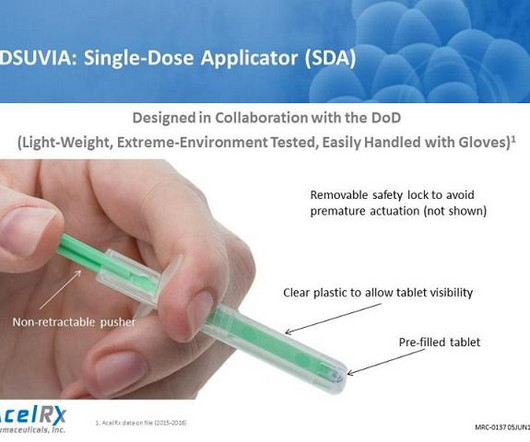
There was a faster onset of analgesia and both higher patient and nurse satisfaction scores with the SSTS as measured by validated questionnaires. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia? What Are the Common Anesthesia Medications?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content