This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
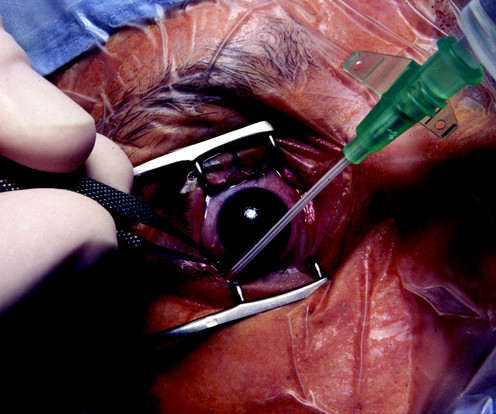
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. The average internal diameter of the radial artery is 1.2 ± 0.3
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality. Yes, it does.
A recent 2024 publication in JAMA looked at 8429 surgical procedures from March 2021 to December 2022 in a single institution. Of course none of the anesthesiologists or operatingroom personnel are dishonest, but preventing theft of these small valuable devices would be difficult. Will I Have a Breathing Tube During Anesthesia?
Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10. Then we’ll roll down the hallway into the operatingroom. You may have nausea after generalanesthesia.
It’s not infrequent that autistic patients need surgery and anesthesia. Patients with autism commonly need to be sedated for routine procedures that a normal child or adult would cooperate with. They told the mother she had the choice of going home without any surgical procedure or anesthesia at all. mg/kg midazolam, and.02
Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. The Anesthesia Consultant’s 2022 List of the Top Anesthesia Books includes: Miller’s Anesthesia , 9th edition, 2019, Editor-in-Chief Michael Gropper.
Between them, Larson and Jaffe have taught hundreds of anesthesia residents the finer points of clinical care. Now, because of this book, readers can find on the printed page what the authors taught in the preoperative forum, in the operatingroom, and in the post-anesthesia recovery room. Together, Drs.
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. If the procedure was an outpatient surgery, you will leave the facility and return home after you’ve recovered from anesthesia.
How will astronauts conduct generalanesthesia and surgery in outer space? If an astronaut requires generalanesthesia, one must assume the patient has a full stomach and is at risk for aspiration. Studies on Earth show that an average of 20 procedures are required to reach a learning curve plateau.
Allow more procedures to be performed When surgery times are shortened, surgeons and other surgery providers are able to work with more patients per day. This means that more procedures are performed, and more patients are assisted overall. Depending on the specialty, around 8 to 10 small surgeries are possible each day.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. Plan: cleared for generalanesthesia providing ECG and labs are normal. The primary care doctor should not estimate the percentage of survival or morbidity for the scheduled procedure.
Shortly after, the spinal anesthetic wore off and the patient was quickly placed under generalanesthesia. The procedure was completed uneventfully after the surgeon, Dr. Annuloplasty, unscrubbed to sucker punch Dr. Millerstein. Dr. Annuloplasty remains in a ketamine-induced haze in the corner of the operatingroom.
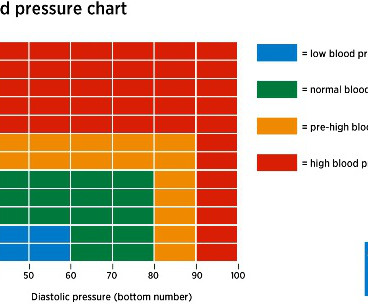
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Predictors of hypotension after induction of generalanesthesia Anesth Analg. Her blood pressure is 150/90 on admission.
In addition, barotrauma occurred in 32% of CICO emergency procedures. Enlisting the surgeon’s help during the procedure is advisable. Dr. Bradley explained that in one approach in Britain, a two-person team traveled from operatingroom to operatingroom to teach the SBT method.
The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site. Assistant surgeon(s) and techs stand at the patient’s side, watch the surgery on video screens, and assist during the operation.
Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. There will be a paucity of new drugs to change the practice of operatingroomanesthesia.
Learn to perform medical procedures at the highest level. Some surgeons are bullies, and are condescending in their remarks and attitudes toward the anesthesia provider they’re working with. The other medical professionals in the operatingroom will respect you for it. Anesthesiologists are hands-on doctors.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% You discuss the procedure of a blood patch and he says, “Yes, that’s what I need.
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. This includes avoiding procedures that cause major pain, bleeding, or disruption of physiology.
Let’s discuss an elephant in the room of operatingroomanesthesia–the association between peripheral nerve blocks and nerve injury. The use of peripheral nerve blocks has crescendoed in anesthesia practice, stimulated by the use of ultrasound-guided visualization of nerves. Liu SS, et al.
This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals. From the exam room to the operatingroom, doctors today follow a clear set of protocols that Dr. Gawande helped establish. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Procedural specialties such as surgery and anesthesiology are higher paying than primary care specialties such as internal medicine or pediatrics. The work of procedural physicians requires specialized skills, and their work incurs more risk than interviewing and examining patients in a clinic.
At times urgent procedures are delayed until the patient has been fasting for 6 hours, and has an appropriate NPO status. Let’s assume your surgeon is determined to operate urgently, and doesn’t want to wait 6 hours after the patient’s meal. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Physicians see EPIC as a software system designed to make billing efficient for the hospitals, so that the hospitals can capture a charge for every dose of medication and every procedure. As an anesthesiologist in the operatingroom, you will have your own EPIC computer next to the anesthesia machine.
iControl-RP is connected to the NeuroSENSE EEG monitor, the two infusion pumps for separately controlled propofol and remifentanil administration, and the operatingroom patient vital signs monitor. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
Pursue a career as an acute care doctor if you prefer adrenaline-charged arenas such as the operatingroom, the intensive care unit, the labor and delivery suite, or the emergency room. Physicians who do procedures, and who incur the risks of procedures gone wrong, earn more money. Income differences.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? I tried it on several of my patients who had prolonged awakening after generalanesthesia.
Just before the start of anesthesia, a patient may hear the operatingroom nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient. Love it or hate it, the EMR is here to stay.
Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. Most of the time an anesthesiologist works in the operatingroom. A busy surgeon may work in the operatingroom two or three days per week. Operatingroom medicine requires action.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). The procedure lasted only 15 minutes. Extubation is risky business.
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Potent inhalation anesthesia (sevoflurane). What do you do?
I work in a private practice setting in Palo Alto, California, and liposuction is one of the most common plastic surgery procedures performed. Early in my career, in the late 1980’s, liposuction was a bloody procedure. Preanesthetic assessment and patient selection are key for safe large-volume liposuction procedures.
Propofol infusions are typically used to make our patients sleep, and most propofol infusions cross the American Society of Anesthesiologists line into generalanesthesia. You may make the surgeon happy, and you may continue to have a safe airway under generalanesthesia in the absence of the endotracheal tube, but what if you don’t?
Dr. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operatingroom. We extended the apnea times of 25 patients with difficult airways who were undergoing generalanesthesia for hypopharyngeal or laryngotracheal surgery. His airway exam shows a thick neck (circumference 42 cm, or 16.5
Daniel Sessler, one of the world’s most respected and prolific anesthesia researchers , is a co-author of the recent Anesthesiology study. To me this validates the notion that continuous finger-cuff technology may eventually gain widespread adoption in operatingroom monitoring. Will I Have a Breathing Tube During Anesthesia?
I don’t tout myself as an expert in AI technology, but I am an expert in taking care of patients, which I’ve done in clinics, operatingrooms, intensive care units, and emergency rooms at Stanford and in Silicon Valley for over 30 years. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operatingrooms/intensive care units. Why Did Take Me So Long To Wake From GeneralAnesthesia?
In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. The ICU attendings had respectful peer relationships with all the surgeons, including the private-practice cardiac surgeons whose post-operative patients were housed in the ICU.
An operatingroom emergency is not a time for screaming, temper tantrums, or freezing. An operatingroom emergency is a time for calm, assertive action. One day I brought my 15-year-old son into the operatingroom with me to observe surgery, hoping he would respect the complex nature of my job.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content