This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Just before the start of anesthesia, a patient may hear the operating room nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? Intravenous caffeine post-surgery is not a new idea. billion dollars by 2024.
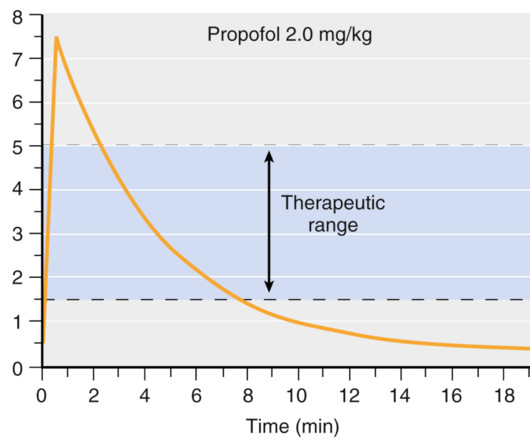
How long will the anesthesia last?” The query “How long does generalanesthesia last?” Intravenous anesthesia is well discussed in the textbook Miller’s Anesthesia , Ninth Edition , Chapter 23. Inhalational anesthesia is well discussed in the textbook Miller’s Anesthesia , Ninth Edition , Chapter 20.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. I’ve performed countless general anesthetics for surgeries requiring smooth emergence, specifically carotid endarterectomies, rhinoplasties, facelifts, craniotomies, thyroidectomies, and other head and neck procedures.
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
I’m writing this review to inform anesthesia providers and laypersons regarding developments in the field of anesthesiology. Vladimir Nekhendzy, Clinical Professor of Anesthesiology and Otolaryngology, Stanford University School of Medicine, and Past President of the Society for Head and Neck Anesthesia, is the inventor of the Spiro device.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
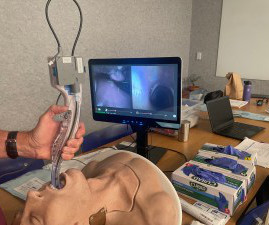
In the smart glasses group, the ultrasound machine was located behind the operator, and the smart glasses were paired with the ultrasound machine. Would the addition of smart glasses for routine monitoring be an overdose of technology in the operating room cockpit? Does excessive technology distract us from the actual patient?
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
For non-anesthesiologists, who will not undergo three years of anesthesia residency training to become DL experts, learning video laryngoscopy instead of direct laryngoscopy makes sense. Of course none of the anesthesiologists or operating room personnel are dishonest, but preventing theft of these small valuable devices would be difficult.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The patient consents.
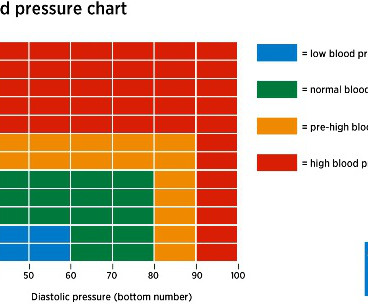
Anesthesia plays a critical role in cesarean sections, not only to ensure the mother’s comfort and pain-free experience but also to safeguard her physiological stability and promote a positive initial bonding with the baby. However, spinal anesthesia can cause hypotension (low blood pressure), which might reduce blood flow to the fetus.
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct generalanesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
Anesthesia has been described as 99% boredom and 1% panic. Careercast.com listed the T op 10 Most Stressful Jobs in America in 2015 , and those jobs were: Firefighter Enlisted Military Personnel Military General Airline Pilot Police Officer Actor Broadcaster Event Coordinator Photo Journalist Newspaper Reporter. Picture a 3 a.m.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operating room? Why Did Take Me So Long To Wake From GeneralAnesthesia?
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operating room.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
CardioPulmonary Resuscitation in the Operating Room The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operating room. Both were published in the journal Anesthesia and Analgesia.
This technique induced vasoconstriction and resulted in decreased blood loss, and made transfusion and post-operative anemia rare. The procedures are done under general endotracheal anesthesia, and can last from 3 to 8 hours. Our facility, the Plastic Surgery Center in Palo Alto, has two operating rooms.
Anesthesiologists are likely to have: A preference for being in an operating room rather than in a clinic. Most of the time an anesthesiologist works in the operating room. A busy surgeon may work in the operating room two or three days per week. A busy anesthesiologist will be in the operating room five or more days per week.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
It’s a fact that cutting a child out from his mother’s womb was a death sentence for the mother in an era prior to the discovery of anesthesia and prior to the discovery of surgical techniques to control bleeding and infection. In emergency circumstances, generalanesthesia may be required for Cesarean section.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
Patients sometimes say, “Why did it take me so long to wake up after anesthesia?” Certain patients have consistent bad experiences from a past general anesthetic. They wonder if they are at increased risk for anesthesia, if something went wrong in their past anesthetics, and whether they can do about it.
You’ve graduated from a residency program in which you learned the nuances of preoperative, intraoperative, and postoperative anesthesia practice. You believe the patient is high risk in terms of his airway, his breathing, his cardiac status, and his potential for post-operative complications. You’re in charge of the anesthetic.
Prior to the machine, it was impossible to successfully operate on the heart while it was still beating. In 1953 he performed the first successful operation on a human using the heart-lung machine. Prior to the arthroscope, this surgery required the surgeon to open the joint to operate directly on the meniscus.
Anesthesiologists still work in hospital operating rooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. Careers in anesthesia are intellectually stimulating, emotionally gratifying, and have high median salaries and ultra-low unemployment.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operating room. Read my column on bullying in the operating room. Hold your heads high.
I ask this question when I’m teaching anesthesia residents and medical students. Control of the airway is the most important clinical priority in anesthesia care. The INTUBATION AFTER INDUCTION OF GENERALANESTHESIA section of the Difficult Airway Algorithm is bifurcated into two pathways. Their most frequent answer is.
Shorten surgery times According to the Canadian Journal of Surgery, operations involving skilled surgical assistants are completed 30 percent faster. Prolonged operative durations can be associated with complications. Shortening your surgery time is critical when considering patient outcomes.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room.
The capacity to deliver this much oxygen to a non-intubated patient is a marked advance in anesthesia care. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operating room. Widespread adoption of HFNO as routine therapy in the operating room is still lacking. I was—in a word—flabbergasted.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operating room suite. All anesthesia providers should have access to the current two-volume 3112-page edition.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
The first was the amount of hypotension during the 15 minutes following the induction of anesthesia, and the second was the time-weighted average MAP less than 65 mmHg during the entire surgery. These parameters provide additional information which, if validated, can expand the information an anesthesia provider can monitor routinely.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content