This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Anesthesia vitalsigns monitor display A second and more compelling use for smart glasses would be the display of a patient’s vitalsign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vitalsign electronic monitors.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. The post What is an OR Nurse and What Do They Do in the OperatingRoom? and Virginia.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. You take the elevator to the third floor and proceed to the locker room.
Secure platforms can provide updates on the progress of the surgery, reducing anxiety and fostering a sense of connection for loved ones waiting outside the operatingroom. Imagine seamlessly reporting pain levels or other vitalsigns through a user-friendly app. Digital tools can also enhance post-surgical care.
Vigilance regarding a sleeping patient’s vitalsigns was always paramount, but the constant effort to be vigilant could be mind-numbing. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). It’s also not uncommon for the patient to be breathing room air during transport.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents. Can this scenario occur?
Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operatingroom 13 of Stanford University Hospital. Upon arrival at the airport in the donor city, an ambulance transported us to the hospital.
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. What do you do? How do you feel about all this?
An anesthesia machine, with the vitalsigns monitor screen on the left, and the electronic medical records computer screen on the right. His vitalsigns are heart rate = 100, BP = 150/80, respiratory rate = 20 breaths/minute, oxygen saturation 95% on room air, and temperature 100.2 The BP is 100/50.
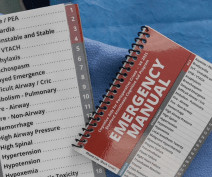
Your patient’s vitalsigns are dropping. You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operatingroom emergencies. A copy of the Manual hangs in every operatingroom at Stanford Hospital.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. A printable version of the Stanford Emergency Manual is available online for free.
Such cases sometimes present to a pediatric hospital for anesthetic care, but at times the child will be treated in a dental office. At this point, the anesthesiologist can take the patient away from the parent and proceed into the operatingroom, where either an intravenous anesthetic or an inhaled sevoflurane anesthetic can be initiated.
A typical hospital will have dozens of other anesthesia providers working in the same building. In an anesthesia care team, a physician anesthesiologist supervises up to four operatingrooms and each operatingroom is staffed with a certified registered nurse anesthetist (CRNA). at a community hospital.
Maggie is paralyzed from the neck down— a ventilator-dependent quadriplegic—and is hospitalized in a private room. Then he injects her IV with a syringe of adrenaline, and leaves the vitalsigns monitor on. The vitalsigns monitor shows her heart rate suddenly change to zero as she dies. Remarkable!
In July 1984 during the first week of my Stanford anesthesia residency at the Santa Clara County Hospital, the entire medical center owned only three Nellcor pulse oximeters. The remaining operatingrooms would proceed without oximetry. Today you can purchase a tiny finger oximeter from Walmart for $11.95
With influenza illness may range from mild to severe and even death, but hospitalization and death occur mainly among high risk groups such as elderly patients or those with preexisting chronic illnesses. That is the real scare of the coronavirus issue—the fear that our hospitals could not handle the volume of severe infections.
Monitoring Patient Condition : Cardiovascular perfusionists must continually monitor the patient’s vitalsigns and respond to any changes that may occur during the procedure. Hospitals and surgical centers rely on perfusionists to support their cardiac surgery teams.
What about monitors of vitalsigns? The standard monitoring devices of pulse oximetry, end-tidal CO2 monitoring, and other essential anesthesia vitalsign monitors were developed and in use by the 1990s. Anesthesia in 2018 is markedly different from anesthesia in the 1990s.
Such clinics can increase operatingroom efficiency and decrease day-of-surgery cancellations and delays, and are especially important prior to major inpatient surgeries such as brain surgeries, chest surgeries, abdominal surgeries and major transplants.
In operatingroom anesthesia, the narcotic fentanyl is a clear liquid usually marketed in vials of two milliliters or five milliliters. An ICU physician will write an order for the dosing of intravenous fentanyl, and the ICU nurse will be in constant attendance to monitor the patient’s vitalsigns and level of sedation.
When I first went into the private practice of anesthesia in 1986, gray-haired anesthesiologists at our community hospital in Fremont, California occasionally injected 100 mg of caffeine into a patient’s IV after a surgery if the patient was slow to wake. “It 6 It’s too soon for caffeine use to become routine in the operatingroom.
This includes basic qualifications like taking blood pressure, vitalsigns, measuring heart rate, and listening with a stethoscope. Some hospitals require 1-2 years of ICU or Critical Care experience in order to be hired. View surgical services/operatingroom RN Sample Resume 8.
Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operatingrooms/intensive care units. What will an AIM robot doctor look like?
A total of 266 cases of brain damage or death during anesthesia care in the operatingroom under the care of a solo anesthesiologist occurred. I refused to staff the case, and told him, “Cases like this—that’s why we have hospitals.” The surgeon needs to know if the vitalsigns are deteriorating.
His hospital chart shows no past anesthetics, and he has no medical problems except hypertension which is treated with lisinopril. His vitalsigns are normal, and his oxygen saturation is 96% on room air.You are six months out of anesthesia training and new to this hospital. What went wrong here?
Tell the surgeon that the patient needs to have cardiac clearance prior to any general anesthetic, and that the case needs to be done in a hospital setting rather than at a freestanding surgery center. I’d like to do this procedure in my office operatingroom, not in a surgery center or the hospital.”
Imagine you’re two months out of anesthesia training, working at a community hospital, and at 2 a.m. The surgeon is not “the captain of the ship” in the operatingroom. Your note should record the timeline, the vitalsigns the patient had, and what your presumed diagnosis was. This observation is no surprise.
The first public demonstration of anesthesia, at the Ether Dome in Massachusetts General Hospital Important advances in the history of anesthesia changed medicine forever. Dr. Morton performed the first public demonstration of general anesthesia at Harvard’s Massachusetts General Hospital on October 16, 1846. Dr. Charles Suckling.
In contrast, other operatingroom professionals are usually relaxed and winding down at this time, because the surgical procedure is finished. She walked out of the hospital two days later. The patient’s vitalsigns remained normal and the ET tube was removed. If the patient has an ET tube, it is usually removed.
Here are some general steps that might be considered: Alert the medical team: The anesthesiologist or healthcare providers in the operatingroom need to be notified immediately about the patient’s deteriorating condition. The surgeon and additional medical personnel may also be called upon for assistance.
His preoperative vitalsigns were normal with an oxygen saturation of 98%. His preoperative vitalsigns were normal. He walked out the hospital alive and well. A 40-year-old male presented for outpatient septoplasty surgery. An endotracheal tube was easily placed, and breath sounds were equal bilaterally.
I was still vibrating from my day in the operatingroom. Get your ass out of that windowless tomb of an operatingroom and take your son back to your childhood home.” I didn’t have a 42-inch monitor displaying Johnny’s vitalsigns, but I knew my son’s blood pressure was escalating. Johnny’s 17 years old.
All four reach the surface, alive and anesthetized, and are transported to a nearby hospital. in an operatingroom by an anesthesiologist) or into a muscle (e.g. No one monitored the vitalsigns of the boys during their 3-hour underwater general anesthetics. sevoflurane), or intravenously. in a cave in Thailand).
Why Data Across the Surgical Continuum Matters Integrated operatingrooms have reshaped surgery in the past decade, providing amongst other benefits, enhanced communication, shortened surgical times, reduced patient cancellations, real-time access to patient information and advanced imaging, as well as maximum use of operatingrooms.
Electronic Medical Records (EMR) in the operatingroom. Today hospital anesthesia medical records are recorded into computer software. The addition of automated drug supply cabinets in the operatingroom was a significant advance over the Sears Craftsman carts we used previously. The result has been a mixed bag.
You learn to inject propofol and intubate a patient in the first few months, but its a lifetime journey to master the medical aspects of evaluating and treating the heart, lungs, brain, kidneys and vitalsigns during anesthesia care. The goal is to be a perioperative (around the time of operation) doctor, not a technician.
Surgery is at the core of any hospital in America, where life-altering decisions are made, and complex procedures are performed under immense pressure. AI has already had an impact across other elements of the hospital revenue cycle model, from patient intake and routing to post-discharge follow-up and care pathways.
These professionals handle a variety of tasks, including performing preoperative assessments, assisting in the operatingroom, and managing postoperative care. Surgical PAs work in various medical settings, such as hospitals, outpatient surgical centers, trauma centers, and specialty surgical clinics.
The text read: 911 call me I was administering an anesthetic to a 41-year-old woman in an operatingroom at Stanford University, while a neurosurgeon worked to remove a meningioma tumor from her brain. I scanned the operatingroom monitors and confirmed that her vitalsigns were perfect. Mom is so pissed.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content