This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In contrast to other APRNs, CRNAs are specially trained to provide anesthesia to patients in settings such as hospitals, clinics, private practices, and doctors’ offices. They also monitor vitalsigns throughout anesthesia, assist patients with recovery and side effects, and conduct post-procedure evaluations.
Anesthesia vitalsigns monitor display A second and more compelling use for smart glasses would be the display of a patient’s vitalsign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vitalsign electronic monitors.
Imagine seamlessly reporting pain levels or other vitalsigns through a user-friendly app. Beyond the Operating Room: Digital Tools Enhance Surgery Day The road to recovery doesn’t end when you leave the hospital. Remote monitoring tools powered by wearable devices can track vitalsigns and recovery progress.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). The hospital supplies oxygen tanks on every gurney used to transport surgical patients from the OR to the PACU.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. Your hospital contains multiple operating rooms, and today you are in room #10.
On physical exam, her vitalsigns are normal, her lungs are clear, and her heart exam is positive for the clicking sound of a mechanical valve and a 2/6 systolic murmur. Vitalsigns remain normal with BP=110/70, P=80, and oxygen saturation=99%. She is obese, weighing 200 pounds, with a BMI=35. She is on no medications.
An anesthesia machine, with the vitalsigns monitor screen on the left, and the electronic medical records computer screen on the right. His vitalsigns are heart rate = 100, BP = 150/80, respiratory rate = 20 breaths/minute, oxygen saturation 95% on room air, and temperature 100.2 Dr. A meets Mr. Doe and interviews him.
Assisting During Surgery : During the procedure, OR nurses work closely with the surgical team by passing instruments, keeping the area sterile, and monitoring the patient’s vitalsigns. Once you’ve gained experience and completed your training, consider signing up for shifts as an OR nurse with Platinum Medical Staffing.
Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operating room 13 of Stanford University Hospital. Upon arrival at the airport in the donor city, an ambulance transported us to the hospital.
Hospital emergency rooms have no shortage of drunken individuals who’ve been involved in motor vehicle trauma, motorcycle accidents, gang violence, or domestic violence. Let’s look at the risks for an acutely alcohol intoxicated patient first. cannabis REF) are present. As a patient, what should you do?
The initial vitalsigns are an oxygen saturation of 95%, heart rate of 90, respiratory rate of 24, and blood pressure of 140/88. The paramedics are onsite, the patient has been reintubated, and the patient is being transported to a nearby hospital. Four liters/min of oxygen are administered intranasally.
Acute dialysis nurses provide dialysis treatments in the hospital to patients with new-onset kidney failure. They also provide treatments to previously established dialysis patients in the hospital. In the hospital, dialysis treatments are provided one-on-one or in a dialysis treatment room.
These should: Cover various types of surgeries, procedures and anesthesia techniques Include preoperative assessments, intraoperative events, drug administration, vitalsigns, fluid balance and postoperative recovery data Enable easy capture, storage and retrieval of relevant patient information 3.
Vigilance regarding a sleeping patient’s vitalsigns was always paramount, but the constant effort to be vigilant could be mind-numbing. Every hospital operating room is equipped with a computer connected to the internet. You’re allowed to bring along a briefcase or a backpack. Love it or hate it, the EMR is here to stay.
Maggie is paralyzed from the neck down— a ventilator-dependent quadriplegic—and is hospitalized in a private room. Then he injects her IV with a syringe of adrenaline, and leaves the vitalsigns monitor on. The vitalsigns monitor shows her heart rate suddenly change to zero as she dies. Remarkable! Coma (1978).
What about monitors of vitalsigns? The standard monitoring devices of pulse oximetry, end-tidal CO2 monitoring, and other essential anesthesia vitalsign monitors were developed and in use by the 1990s. The adage that “the patient comes first” is sometimes lost in an array of LED displays, passwords, and keyboards.
Such cases sometimes present to a pediatric hospital for anesthetic care, but at times the child will be treated in a dental office. MONITORING THE PATIENT: The patient should have all the same monitors an anesthesiologist would use in a hospital or a surgery center. The anesthesiologist is the main monitor.
Medical-Surgical Nursing is the Foundation of Hospital Nursing Medical-Surgical Nursing is the foundation of hospital nursing. Delegation of tasks such as vitalsigns and blood glucose monitoring is necessary. This record also serves as the primary form of communication between all hospital departments.
This includes basic qualifications like taking blood pressure, vitalsigns, measuring heart rate, and listening with a stethoscope. Some hospitals require 1-2 years of ICU or Critical Care experience in order to be hired. Click here to view our Dialysis Registered Nurses Resume Example 9.
When I first went into the private practice of anesthesia in 1986, gray-haired anesthesiologists at our community hospital in Fremont, California occasionally injected 100 mg of caffeine into a patient’s IV after a surgery if the patient was slow to wake. “It The market share for leading energy drink brands is shown below. It helps a lot!”
Monitoring Patient Condition : Cardiovascular perfusionists must continually monitor the patient’s vitalsigns and respond to any changes that may occur during the procedure. Hospitals and surgical centers rely on perfusionists to support their cardiac surgery teams.
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. Alerts or abnormal vitalsigns and laboratory results are represented by squares and triangles, respectively.
Your day could consist of ensuring clear and concise communication with patients as you educate them on a variety of topics, taking vitalsigns, wound care, removing staples, relaying findings to the doctor, charting on a computer system, etc.
With influenza illness may range from mild to severe and even death, but hospitalization and death occur mainly among high risk groups such as elderly patients or those with preexisting chronic illnesses. That is the real scare of the coronavirus issue—the fear that our hospitals could not handle the volume of severe infections.
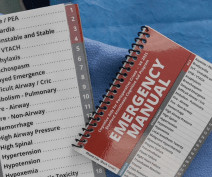
When a Code Blue or a dire change in vitalsigns occurs in an operating room, the Manual directs the resuscitation team to the correct order of action at a time when minds are racing, thoughts have become jumbled, and near-perfect intervention is required.
In July 1984 during the first week of my Stanford anesthesia residency at the Santa Clara County Hospital, the entire medical center owned only three Nellcor pulse oximeters. The oxygen saturation became recognized as “the fifth vitalsign,” joining heart rate, blood pressure, respiratory rate, and temperature.
You can choose short-term or long-term contractual assignments and pick from various settings, from small-town clinics to large teaching hospitals and everything in between. Today’s L&D nurse might work in a hospital L&D unit, a physician’s office, or a maternity or birthing center. an hour.
Your patient’s vitalsigns are dropping. A copy of the Manual hangs in every operating room at Stanford Hospital. An anesthesia emergency occurs without warning. As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient.
His hospital chart shows no past anesthetics, and he has no medical problems except hypertension which is treated with lisinopril. His vitalsigns are normal, and his oxygen saturation is 96% on room air.You are six months out of anesthesia training and new to this hospital. What went wrong here?
How soon will we see robotic anesthesia in our hospitals and surgery centers? Most of these discoveries originated in Silicon Valley, just miles outside Stanford University Hospital where I’ve been working for the past 42 years. Our medical world inside the hospital has changed more slowly. Relatively little.
The physical exam includes the height, weight, vitalsigns, and documentation of any abnormal findings on exam of the entire body. The primary care doctor should not recommend where the surgery should or should not be done, e.g. in a hospital, a surgery center, or in a doctor’s office.
A typical hospital will have dozens of other anesthesia providers working in the same building. In a university hospital, a faculty member may supervise two operating rooms each with a resident anesthesiologist-in-training in attendance. at a community hospital. This is when the free-soloing begins. Sound scary? Sound scary?
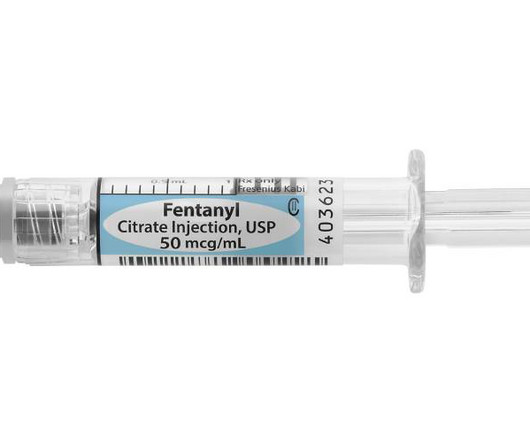
An ICU physician will write an order for the dosing of intravenous fentanyl, and the ICU nurse will be in constant attendance to monitor the patient’s vitalsigns and level of sedation. After surgery, hospital inpatients who have postoperative pain are typically treated with longer acting narcotics such as morphine or Dilaudid.
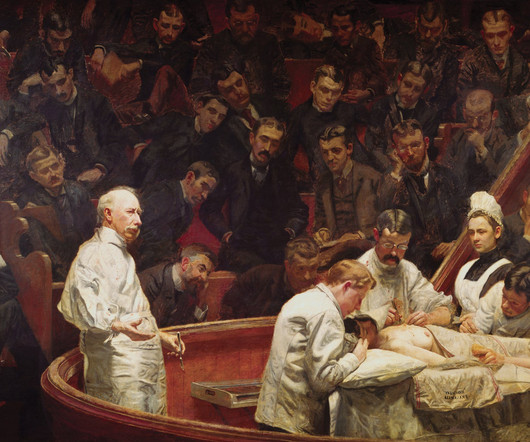
The first public demonstration of anesthesia, at the Ether Dome in Massachusetts General Hospital Important advances in the history of anesthesia changed medicine forever. Dr. Morton performed the first public demonstration of general anesthesia at Harvard’s Massachusetts General Hospital on October 16, 1846. Dr. Archie Brain, England.
Intraoperative monitoring involves the use of specialized equipment and techniques to track a patient’s vitalsigns and neurological functions throughout a surgical procedure. This leads to shorter hospital stays and a quicker return to normal activities for patients.
AI computers will be stocked with information from multiple sources, including all known medical knowledge published in textbooks and journals, as well as the electronic health records (EHR)/ clinical data from thousands of previous hospital and clinic patients.
His preoperative vitalsigns were normal with an oxygen saturation of 98%. His preoperative vitalsigns were normal. He walked out the hospital alive and well. A 40-year-old male presented for outpatient septoplasty surgery. An endotracheal tube was easily placed, and breath sounds were equal bilaterally.
I refused to staff the case, and told him, “Cases like this—that’s why we have hospitals.” There are pressures to perform increasingly difficult procedures on increasingly sicker patients in non-hospital settings. The surgeon needs to know if the vitalsigns are deteriorating. Resist these pressures.
Let’s examine five actual post-extubation scenarios that caused death, complications, or a near-miss: During my first month of anesthesia training at a county hospital in San Jose, California, I chose to try to wake up a healthy patient without the presence of my faculty member. She walked out of the hospital two days later.
Identify and address potential causes: Once the patient’s vitalsigns have stabilized or as the resuscitation efforts continue, the medical team will work to identify the underlying cause of the cardiac event. I’ve had an interest in AI and robots in medicine for years.
Imagine you’re two months out of anesthesia training, working at a community hospital, and at 2 a.m. Your note should record the timeline, the vitalsigns the patient had, and what your presumed diagnosis was. This observation is no surprise. Your third responsibility is to write a detailed note about what happened.
The procedure does not require a breathing tube, so we’ll administer the sedation and be vigilant regarding what happens to the patient’s vitalsigns. Joining the hospital staff, Nico runs afoul of a grouchy nurse anesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
Tell the surgeon that the patient needs to have cardiac clearance prior to any general anesthetic, and that the case needs to be done in a hospital setting rather than at a freestanding surgery center. I’d like to do this procedure in my office operating room, not in a surgery center or the hospital.”
Neither ciprofol nor propofol caused statistically significant differences in vitalsigns. 2022) conducted a phase III study at ten teaching hospitals, comparing ciprofol and propofol for deep sedation for colonoscopy or gastroscopy. Chen et al. 2022) randomized 150 patients to ciprofol or propofol for hysteroscopy.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content