This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There are four classes of APRNs: certified nurse midwife (CNM), clinical nurse specialist (CNS), certified nurse practitioner (CNP), and certified registered nurseanesthetist (CRNA). CNS providers are often involved in educational programs to improve nurse performance, patient outcomes, and bedside nursing.
Securing admission into a Certified Registered NurseAnesthetist (CRNA) program is no small feat. In this blog post, we will dive into the challenges posed by high demand and intense rivalry in CRNA program admissions and explore strategies to overcome them. 5 Strategies to Rise Above the Rivalry 1.
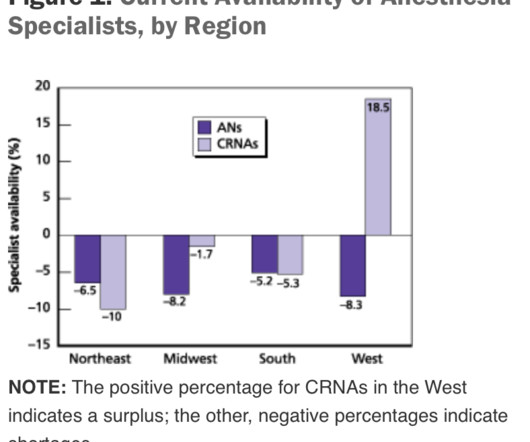
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
s NurseAnesthesia program, sharing their nursing backgrounds and why they were particularly interested in York's program. Phillips-Hill and staff received a demonstration on spinal and intubation procedures, and moved along to the EP Lab to witness some afib ablations. State Senator Phillips- Hill.
3,4 It has been linked to multiple intra-operative and post-operative complications (e.g., greater volatile anesthetic requirement, increased morbidity and mortality rates, and greater pain somatization and post-operative analgesic requirements). 3,4 It has been linked to multiple intra-operative and post-operative complications (e.g.,
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. Proper planning creates the best possibility for surgical procedures to go well.
Anesthesiology is a wonderful profession, as I have described in many previous posts on theanesthesiaconsultant.com. But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. Anesthesia providers are at best consultants, and at worst, “worker bees” called upon to provide a service.
Will it be a nurse or will it be a physician? A 2013 study in Anesthesiology states, “Despite the fact that a surgical procedure may have been performed for the appropriate indication and in a technically perfect manner, patients are threatened by perioperative organ injury. This is an important question. Why do patients die?
Certified Registered NurseAnesthetists (CRNAs) are advanced practice registered nurses (APRNs) who provide anesthesia related care in a variety of healthcare settings before, during, and after therapeutic, diagnostic, surgical, and obstetrical procedures.
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. binocular Moverio BT-35E smart glasses A South Korean group led by Dr. Y.E.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. I’m writing this in January 2016.
Does exposure to general anesthesia cause dementia? Association of Mild Cognitive Impairment With Exposure to General Anesthesia for Surgical and Nonsurgical Procedures: A Population-Based Study. All of their anesthesia records for surgeries after the age of 40 were reviewed. In a word, “No.” Anesthesiology.
Growing shortages of anesthesiologists globally could significantly impact the availability of surgeries and other medical procedures, especially in rural and low-income areas. A looming shortage of anesthesiologists globally may affect the accessibility of healthcare in the next ten years. million operations from taking place (3).
GENERAL ANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation. What do you do?
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The surgery concludes at 1630 hours.
What should you do if your 2-year-old son or daughter requires surgery and anesthesia? Discuss with parents, caregivers, and pregnant women the benefits, risks, and appropriate timing of surgery or procedures requiring anesthetic and sedation drugs.” What are the anesthetic risks for children? Should you consent to proceed?
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
I work in a private practice setting in Palo Alto, California, and liposuction is one of the most common plastic surgery procedures performed. Early in my career, in the late 1980’s, liposuction was a bloody procedure. Preanesthetic assessment and patient selection are key for safe large-volume liposuction procedures.
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
Regional anesthesia is a growing frontier in modern clinical anesthesia, in part because of the availability of ultrasonic imaging to help us direct needle placement. The subspecialty of regional anesthesia has blossomed. following general anesthesia in contrast to a peripheral nerve injury rate of 1.7% Low, but not zero.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
During this COVID crisis, intensive care unit and emergency room doctors and nurses in hotspots like New York City have dangerous, exhausting jobs keeping coronavirus patients alive. A minority of doctors and nurses are saddled with these dangerous around-the-clock jobs battling the disease in ICUs and ERs.
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 A surgical airway is an invasive airway via the front of the patient’s neck into their trachea.
Anesthesia is a hands-on specialty. Anesthesia is said to be “99% boredom and 15 panic,” because 99% of the time patients are stable, yet 1% of the time, especially at the beginning and the end of anesthetics, urgent or emergency circumstances could threaten the life of the patient. Love it or hate it, the EMR is here to stay.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
One goal of theanesthesiaconsultant.com is to make the practice of anesthesia safer. The practice of anesthesia on healthy patients is quite safe, but we want to do everything we can to avoid preventable errors. The safety of anesthesia on ASA I and II patients has been compared to the safety record of commercial aviation.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The ET tube is a conduit to safely transfer oxygen and anesthesia gases into and out of the lungs. Extubation is risky business.
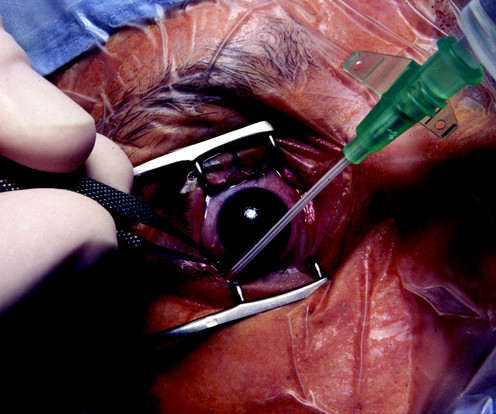
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. You are on call for the repair. What do you do? Discussion: There are two issues.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. The surgical attendings were the kings, the students were the peasants, the nurses and techs were serfs, and the anesthesiologists were the whipping boys for the surgeons. Why would I say this? Five minutes later, the patient had a cardiac arrest.
I ask this question when I’m teaching anesthesia residents and medical students. Control of the airway is the most important clinical priority in anesthesia care. The INTUBATION AFTER INDUCTION OF GENERAL ANESTHESIA section of the Difficult Airway Algorithm is bifurcated into two pathways. Their most frequent answer is.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. His question prompted me to write this column. to 25 μg/kg/hr.” “We We commonly administer 1.5
The procedure was to be done in the prone position, and required endotracheal intubation. The patient was turned prone, and the procedure commenced. After only 15 minutes of operating time, the gastroenterologist announced that the procedure was over. The trachea was extubated. The trachea was extubated.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. Medications may need to be adjusted or temporarily stopped to minimize potential risks during the procedure. This could indicate a cardiac event or a complication related to the anesthesia.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. You take the elevator to the third floor and proceed to the locker room.
Learjet anesthesia? Yes, anesthesia can be a glamorous specialty. Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operating room 13 of Stanford University Hospital.
We’re going to sedate this patient for a medical procedure. The procedure does not require a breathing tube, so we’ll administer the sedation and be vigilant regarding what happens to the patient’s vital signs. Let’s discuss a hypothetical male patient. He is 79 years old, overweight, and has a thick neck.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. I’m fascinated by the topic of artificial intelligence in medicine. This is the third column in a series regarding robots in medicine. Smartphones verbally direct us to our destination through mazes of highways and traffic.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
These alarms would bring a fleet of nurses and/or doctors into the room to try to save the patient. I love the movies, but it can be painful to watch scenes where the facts are distorted, sometimes so much that the storyline is implausible. This film is my Hollywood medical pet peeve, and the movie that motivated me to write this column.
How do you feel when you meet your anesthesia provider prior to a surgical procedure? In an abstract presented at the 2015 American Society of Anesthesiologists annual meeting, data from the 2014 National Anesthesia Clinical Outcomes Registry was compiled for every anesthesiologist of known age who performed at least 100 cases.
It’s vital that your stomach is empty prior to elective surgery and anesthesia. Under anesthesia these reflexes are absent. These fasting guidelines do not apply to surgical procedures under local anesthesia, or to those with no anesthesia. Once you’re anesthetized, your cough reflex and gag reflex are abolished.
Can anesthesia machines be used as ICU ventilators for COVID-19 patients? Every anesthesia machine has a ventilator attached to it. For years physician anesthesiologists have transported sick patients from the intensive care unit (ICU) to the operating room (OR) when patients needed a surgical procedure. Yes, they can.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content