This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What’s the difference between a physician anesthesiologist and a nurseanesthetist? There is no fork in the career path that makes a busy Certified Registered NurseAnesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. The answer: internal medicine.
All APRNs are registered nurses who have earned a graduate degree that certifies them to practice advanced and specialized care. There are four classes of APRNs: certified nurse midwife (CNM), clinical nurse specialist (CNS), certified nurse practitioner (CNP), and certified registered nurseanesthetist (CRNA).
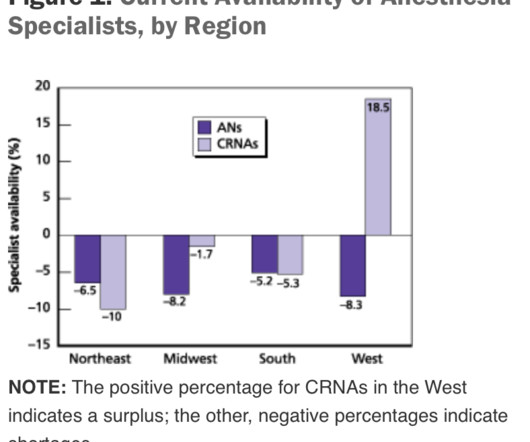
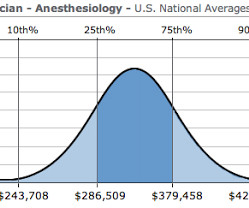
The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurseanesthetists, and 3,200 anesthesiologist assistants. The net decrease in MD anesthesiologists was 2500 – 1900 = 600. Leverage technology.
The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). A quote from the Medscape article read: “Adam Dachman, MD, a surgeon at the hospital, speaking for himself, said he has no problem using nurseanesthetists. (He Why did this change happen?
The benefits of this model are that there are fewer providers involved and less supervision needed. Anesthesia Care Team (ACT) This model incorporates a physician anesthesiologist who supervises CRNAs (certified registered nurseanesthetists), with resident physicians-in-training who ultimately administer the anesthetics.
At times, physician anesthesiologists employ certified registered nurseanesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. In this model, an MD anesthesiologist supervises up to four CRNAs who work in up to four different operating rooms simultaneously. or doctor of osteopathy (D.O.)
No, it’s not the nurseanesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. The hospital plans to replace the doctors with nurseanesthetists. What is this threat?
In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurseanesthetists in multiple operating rooms. Physician anesthesiologists pay their nurseanesthetists as employees as well as their other expenses, and then divide the profit.
If you work in a practice which utilizes an anesthesia care team, where one physician anesthesiologist may supervise, for example, 4 Certified Registered NurseAnesthetists (CRNAs), then a physician’s income is increased because he or she is billing for and supervising care for multiple concurrent surgeries.
In anesthesia care team models, in which a Certified NurseAnesthetist (CRNA) is physically present in the operating room while being supervised by an attending physician anesthesiologist, the MD anesthesiologist can be summoned to return to the operating room in seconds if a problem arises.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone.
In an anesthesia care team, a physician anesthesiologist supervises up to four operating rooms and each operating room is staffed with a certified registered nurseanesthetist (CRNA). In a university hospital, a faculty member may supervise two operating rooms each with a resident anesthesiologist-in-training in attendance.
A physician anesthesiologist supervising four CRNAs in four operating rooms could do four times as many cases per year, so a predicted incidence would be 16-20 cardiac arrests in a 30-year career. A busy anesthesiologist doing his or her own cases performs 1000 anesthetics per year.
Anesthesiologists who supervise Certified Registered NurseAnesthetists (CRNAs) or Anesthesia Assistants (AAs) in an anesthesia care team model often have to provide care for multiple patients simultaneously. These attending anesthesiologists cannot physically be present in multiple operating rooms at all times.
Will your anesthesia professional be a physician anesthesiologist, a Certified Registered NurseAnesthetist (CRNA), or an anesthesia care team made up of both? If an anesthesia care team is attending to you, how many rooms is each physician anesthesiologist supervising?
A supervising attending must teach them, mentor them, and lecture them—case by case—until each resident learns the basic skills. Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
This parallels the original genesis of the role of a nurseanesthetist—to be present during stable phases of anesthetic management—so that the physician anesthesiologist could roam to other operating rooms as needed. What will an AIM robot doctor look like? Google is working on an AIM project in the United Kingdom entitled DeepMind.
Will your anesthesia professional be a physician anesthesiologist, a Certified Registered NurseAnesthetist (CRNA), or an anesthesia care team made up of both? If an anesthesia care team is attending to you, how many rooms is each physician anesthesiologist supervising?
You supervise the rotating of the operating room table 180 degrees, so the patient’s head and airway are adjacent to the anesthesia equipment again. For anesthesiologists, the interval between surgeries is a time when the surgeons, nurses, and the empty operating room are waiting for you to get things going again.
20, 2025 /PRNewswire/ -- Certified registered nurseanesthetists (CRNAs) are usually the last person a patient sees before a surgical procedure begins, and the first person they awake to when it ends. The average nurseanesthetist completes 9,000 clinical hours prior to becoming a CRNA. HARRISBURG, Pa.,
The nurseanesthetist ignored Perpich’s cordial introduction and said nothing to me. He was only a nurseanesthetist. We have six nurseanesthetists, but for tough cases we need an M.D. So the rest of the anesthesia staff is all nurses?” “Yep. Six nurseanesthetists. Bobby Dylan?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content