This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered Nurse Anesthetist (CRNA) is a journey marked by immense growth but also profound challenges. Here’s a closer look at what this transition entails and how the Society of Future Nurse Anesthetists (SFNA) supports aspiring CRNAs in navigating these changes.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. What Does an OR Nurse Do?
Happy CRNA Week 2024 A lot has happened The last two months I moved to San Diego Oh what joyous fun A lot of changes for my family and for me New preschool, grandparent help, New workplace A lot of things to learn “Reprogramming” I’d like to say Each NORA (Non-OperatingRoomAnesthesia) location Different than the next A lot of new people More than (..)
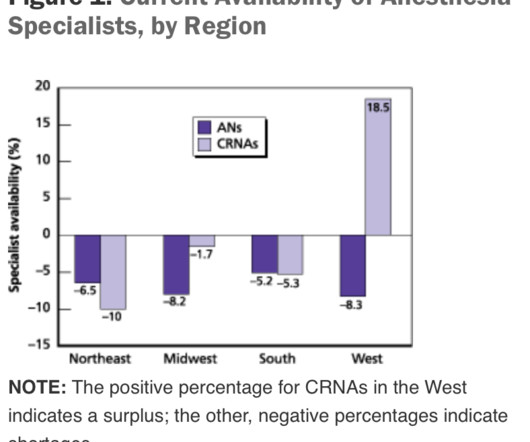
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Just before the start of anesthesia, a patient may hear the operatingroomnurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
When you think of the operatingroom (OR), what comes to mind? I spent more than 40 years working in nursing before joining 3M five years ago. At my first hospital, I visited the nursing director regularly to see if there were any openings. Managing the room, including supplies, equipment, lighting and documentation.
Anesthesia vital signs monitor display A second and more compelling use for smart glasses would be the display of a patient’s vital sign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vital sign electronic monitors. Let me give you a historical perspective.
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. Journal of PeriAnesthesia Nursing, Oct. 24–30, [link] 2.
In the surgery center specifically, Sullivan’s team helped establish an operatingroom committee. Something as simple as changing blocks will affect what rooms will run cases, what different staff segments need to prepare, and what’s available for add-ons. The crux of the issue sat with the incumbent all-nurse staffing model.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Will it be a nurse or will it be a physician? Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model.
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room. PACU nurses contribute significantly to this efficiency.
During this COVID crisis, intensive care unit and emergency room doctors and nurses in hotspots like New York City have dangerous, exhausting jobs keeping coronavirus patients alive. A minority of doctors and nurses are saddled with these dangerous around-the-clock jobs battling the disease in ICUs and ERs.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The patient consents.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Since the development of the internet, anesthesia practice has changed forever.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The video is posted here. The required parts are an operatingroomanesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. Most of the time an anesthesiologist works in the operatingroom. A busy surgeon may work in the operatingroom two or three days per week. Operatingroom medicine requires action.
As a registered nurse, you would think that all this technology supporting the hiring process of nurses would lead to improvements or faster response times but if you have ever spent time on a single application website then you know the frustration and effort that simply goes to waste. What a disaster?!
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
Learjet anesthesia? Yes, anesthesia can be a glamorous specialty. Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operatingroom 13 of Stanford University Hospital.
Anesthesia departments are crucial to the success of operatingrooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. Are we physicians or are we glorified advanced practice nurses?” In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom.
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
Certified Registered Nurse Anesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. To begin, it’s essential to understand the role of a CRNA.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). It’s also not uncommon for the patient to be breathing room air during transport.
When you enter the healthcare facility, a nurse will question you regarding virus symptoms, and will screen you by taking your temperature. The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom? No, they want a skilled practitioner.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
Anesthesiology is a wonderful profession, as I have described in many previous posts on theanesthesiaconsultant.com. But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. In the operatingrooms, the patients are brought in by the surgeons. What is this threat?
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operatingroom.
You’ve found The Anesthesia Consultant website, so you have some interest in anesthesia. The truth is: a career in anesthesia involves unique demands that most people would not seek, tolerate, or ever grow accustomed to. An operatingroom emergency is not a time for screaming, temper tantrums, or freezing.
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurse anesthetist was listed as #11 on the Best Paying Jobs list. What Are the Common Anesthesia Medications?
Advanced Practice Provider Spotlight: Certified registered nurse anesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurse anesthetist (CRNA) at Penn State Health Milton S.
My experience in Quality assurance/Quality improvement programs includes: Stanford University Hospital QA Committee (Care Review Committee), 1997 – 2009 Stanford University Anesthesia QA Committee, 2002 – 2009, and Waverley Surgery Center QI Committee (Chairman), 2002 – present. The first task is to find out about all adverse events.
Each bed would require a ventilator, a set of monitors, and around-the-clock nursing staffing. Can an anesthesia machine in an operatingroom be used as an ICU ventilator? Can an anesthesia machine in an operatingroom be used as an ICU ventilator? Will I Have a Breathing Tube During Anesthesia?
3 Ways Surgical Providers Improve Patient Outcomes Surgical providers—surgical assistants, nurses, and surgical technologists—provide aid during surgery to doctors. Minimize patient time under anesthesia General anesthesia induces a sleep-like state using a combination of intravenous medications and inhaled gasses.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. He’s right. What happened?
An anesthesia machine, with the vital signs monitor screen on the left, and the electronic medical records computer screen on the right. A then records all pertinent preoperative information into the electronic medical record (EMR) via a computer keyboard and screen located just to the right of his anesthesia machine.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency. After ten minutes, he left to pursue other duties.
Fentanyl was introduced in the 1960s when it was first patented under the brand name Sublimaze , and fentanyl quickly became the most commonly administered narcotic by anesthesia providers. In operatingroomanesthesia, the narcotic fentanyl is a clear liquid usually marketed in vials of two milliliters or five milliliters.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content