This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It’s a path that demands not only clinical excellence but also a significant shift in roles—from direct patient care in a high-intensity setting to the precision and autonomy of anesthesia. Understanding the Shift The transition from ICU to operatingroom (OR) involves a fundamental change in responsibilities.
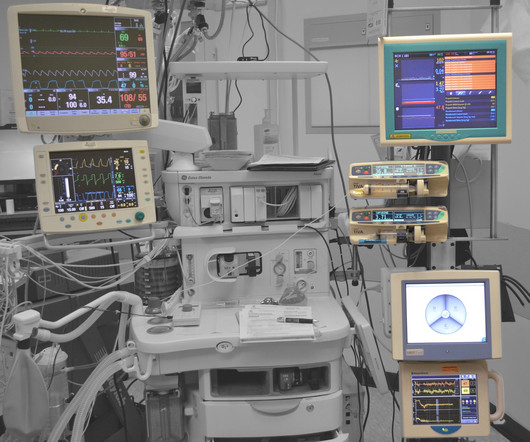
Anesthesia vital signs monitor display A second and more compelling use for smart glasses would be the display of a patient’s vital sign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vital sign electronic monitors. Let me give you a historical perspective.
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. The American Journal of Surgery, vol. 24–30, [link] 2. Arora, Sonal, et al.
Happy CRNA Week 2024 A lot has happened The last two months I moved to San Diego Oh what joyous fun A lot of changes for my family and for me New preschool, grandparent help, New workplace A lot of things to learn “Reprogramming” I’d like to say Each NORA (Non-OperatingRoomAnesthesia) location Different than the next A lot of new people More than (..)
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. The post What is an OR Nurse and What Do They Do in the OperatingRoom?
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
In the surgery center specifically, Sullivan’s team helped establish an operatingroom committee. Something as simple as changing blocks will affect what rooms will run cases, what different staff segments need to prepare, and what’s available for add-ons. OR committees are important for any hospital, HOPD, or ASC.
When you think of the operatingroom (OR), what comes to mind? Managing the room, including supplies, equipment, lighting and documentation. If patient status changes, you may have to switch what you are doing – stepping in to help anesthesia, for example. An intense and stressful work environment?
It’s easier to train non-anesthesiologists (emergency room MDs, critical care internal medicine MDs, EMTs and helicopter trauma RNs) to use VL versus DL. For non-anesthesiologists, who will not undergo three years of anesthesia residency training to become DL experts, learning video laryngoscopy instead of direct laryngoscopy makes sense.
Annual meeting Vice-Chair Dr. Engy Said put together a fantastic point-of-care ultrasound and regional anesthesia workshop on Thursday. Mason as well as some other inspirational anesthesiologists, see these video interviews posted by Dr. Allison Fernandez for the Women of Impact in Anesthesiology project.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The video is posted here. The required parts are an operatingroomanesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operatingroom.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom? Why Did Take Me So Long To Wake From General Anesthesia?
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room.
Anesthesia departments are crucial to the success of operatingrooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
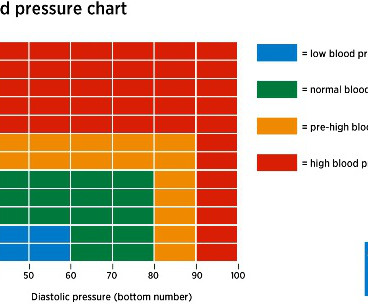
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. You will wear a mask in the preoperative room, and that mask will remain on your face until just prior to the induction of anesthesia.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
The Crucial Role of Surgical Assistants in Plastic Surgery Surgical assistants are indispensable in the operatingroom, handling tasks that are critical to the success of any procedure. Postoperative Care: Assisting with closing incisions, applying dressings, and ensuring patient comfort as they recover from anesthesia.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. ebook $165.29, hardcover $126.17) The Stanford Emergency Manual.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). (He In a word, no. No, they are not.
The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” A score of 40 – 60 is considered an optimal amount of anesthesia depth.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. He’s right. What happened?
Some of their main tasks include: Preparing the OperatingRoom : Surgical assistants ensure all equipment is sterile and ready. Surgical assistants streamline the entire process from pre-op to post-op. This reduces patient time under anesthesia and the risk of complications. We serve Maryland, Washington D.C.,
Photo by Magali Gauthier/The Almanac Between his time in the operatingroom, teaching, and raising his three sons, Atherton resident Dr. Rick Novak has found time to write two novels. The post DOCTOR BY DAY, SCI-FI WRITER BY NIGHT appeared first on The anesthesia consultant.
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. Careers in anesthesia are intellectually stimulating, emotionally gratifying, and have high median salaries and ultra-low unemployment.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
SCALPEL, BOUGIE, TUBE APPROACH TO CRICOTHYROIDOTOMY This week I attended an outstanding Stanford Anesthesia Grand Rounds delivered by Drs. Most anesthesia professionals have never cut into a patient’s neck, but we must own this skill if the necessity arises. Jeremy Collins, Susan Galgay, and Tom Bradley.
Is the practice of anesthesia an art or a science? My career has bridged clinics, operatingrooms, intensive care units, emergency rooms, and helicopter trauma medicine. In the 21 st century operatingroom practice of anesthesiology, we typically have ten minutes to talk to a patient prior to rendering them unconscious.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
Is your doctor an experienced anesthesia provider or a newbie? The list below chronicles the crescendo of growth of as I’ve witnessed it from a newly-trained anesthesia doctor to an expert practitioner. In my view, inexperienced anesthesia providers are more likely to: Be nervous/anxious. This observation is no surprise.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content