This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Anesthesiology residents play an important role in the operating room (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
Post-AnesthesiaCare Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operating room and continues until they are stable enough to recover at home or in a hospital room. Their role in maintaining the flow of operations cannot be overstated.
Anesthesia departments are crucial to the success of operating rooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Lookout for: A trend toward severe post-operative nausea and vomiting.
The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room.
In an operating room, the CRNA administers the anesthesia according to the predetermined plan and monitors the patient’s vitals in order to adjust levels as needed. The CRNA uses a variety of information to execute and modify the anesthesia plan as needed, including measures to assess patient safety and comfort.
You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operating room emergencies. You’re an expert witness or a member of your hospital’s Quality Improvement committee, charged with reviewing the unfortunate outcome of an operating room medical complication.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesiacare unit (PACU). In conclusion, the post-surgical transport of a patient from the operating room to the PACU is a period of patient risk.
No one wants a partner who repeatedly creates conflict in the workplace, who initiates conflict with a surgeon in the operating room, a nurse in the postanesthesiacare unit, or an administrator. Do you think patients want a friendly anesthesiologist who is all thumbs in the operating room?
However, with dozens of stakeholders involved, the pre-anesthesia testing process is anything but simple. To enhance your organization’s process, focus on communications, standard operating procedures and checklists, and interdepartmental accountability.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operating room. If the procedure was an outpatient surgery, you will leave the facility and return home after you’ve recovered from anesthesia.
PREOPOPERATIVE CARE : Let’s talk about the diagnosed sleep apnea patient and pre-operative assessment for upcoming surgery: The diagnosis of OSA is based on the presence of symptoms, such as disturbed sleep, snoring, hypertension, and also the frequency of sleep-related respiratory events during a sleep study or home sleep apnea testing.
Their patients are obtunded on arrival to the PostAnesthesiaCare Unit (PACU) after surgery, and they rely on the PACU nursing staff to complete the job of anesthesia wake up. Some surgeons are bullies, and are condescending in their remarks and attitudes toward the anesthesia provider they’re working with.
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operating room at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. She was extubated one hour later at the surgery center after treatment with diuretic, oxygen, and ventilation via the tube.
The two hospital guards and the mother donned white operating room coveralls. At the mother’s consent, the guards laid the patient down on the hospital gurney, held him there, and the surgical team and the guards pushed the gurney down the hallway to the operating room (a significant distance of approximately 100 yards).
Perioperative” means “the time around an operation”—specifically the preoperative, postoperative, and intraoperative times. Inexperienced anesthesiologists may only contemplate a recipe of anesthesia drugs, instead of seeing his or her role as the management of the patient’s medical problems prior to, during, and after surgery.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesiaCare Unit in excellent condition.
View Critical care RN Sample Resume 7. Operating Room, Perioperative or Surgical Services Resume Example Operating Room Registered Nurses (OR RNs) can be named by various nursing job titles including surgical services registered nurses and/or perioperative registered nurses.
These rotations of an anesthesia resident develop the young doctor into a clinician comfortable in preoperative assessment and management, in the intraoperative administration of anesthesia, and in the postoperative evaluation and treatment of patients.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The patient enters the operating room at 0730 hours. The patient consents. From1985 to 1989, 7.1%
Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
Anesthesiologists are responsible for your medical care before, during, and after surgeries. Perioperative” means “around the time of operations.” A then records all pertinent preoperative information into the electronic medical record (EMR) via a computer keyboard and screen located just to the right of his anesthesia machine.
Dr. Patel has been a pioneer in bringing HFNO/THRIVE from the ICU into the operating room. Widespread adoption of HFNO as routine therapy in the operating room is still lacking. This PEEP effect improves alveolar recruitment, and might also improve gas exchange.
You believe the patient is high risk in terms of his airway, his breathing, his cardiac status, and his potential for post-operative complications. Propofol infusions are typically used to make our patients sleep, and most propofol infusions cross the American Society of Anesthesiologists line into general anesthesia.
Case study #2020: The attending surgeon and the operating room nurse each filed digital Adverse Event documents because of their patient’s extremely high blood pressure and heart rate, and her unplanned admission to the ICU. Case #2020: The surgeon, operating room nurse, and the anesthesiologist are interviewed.
Every time a healthcare provider clicks his or her mouse on an EMR, that click is recorded by the Orwellian Big Brother of Medical Care, the audit trail. An audit trail can be defined as a “record that shows who has accessed a computer system, when it was accessed, and what operations were performed.”
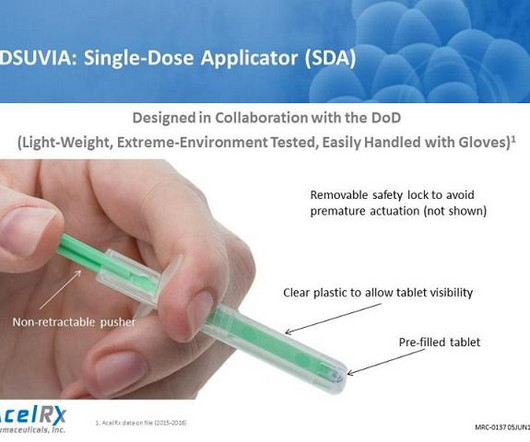
My assessment of sublingual sufentanil, based on the information above, is as follows: Sublingual sufentanil (SS) can be useful in hospitalized post-operative patients following major, painful surgeries such as orthopedic total joint replacements or intra-abdominal surgeries. SS could replace PCA intravenous morphine or fentanyl.
The surgery and anesthesia proceed uneventfully. The patient is awakened from general anesthesia and taken to the PostAnesthesiaCare Unit. Abdominal surgery and general anesthesia in this patient population are not without risk, even with optimal anesthetic care. The patient accepts these risks.
The post-operative recovery room, also known as the post-anesthesiacare unit (PACU), is a critical environment where patients are closely monitored following surgery. Equipped with advanced medical technology that helps safeguard against complications while patients transition from anesthesia to consciousness.
You learn to inject propofol and intubate a patient in the first few months, but its a lifetime journey to master the medical aspects of evaluating and treating the heart, lungs, brain, kidneys and vital signs during anesthesiacare. The goal is to be a perioperative (around the time of operation) doctor, not a technician.
The healthcare landscape is rapidly evolving, demanding innovative approaches to improve patient outcomes and streamline operations. While clinical trials and registries have established the gold standard for the regulatory approval pathway, they fall short in capturing the nuances and complexities of real-world patient care.
Both female and male patients eventually woke up, were sent to the PostAnesthesiaCare Unit, and were ultimately discharged to their hospital room or to their home. For decades we were never aware, we were never taught, nor did we teach, that females recovered from volatile anesthetic faster than males.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content